Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
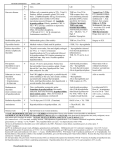
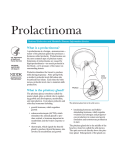
Endocrine (2-12-99) Hypopituitarism: Causes: Ischemic necrosis Ex - postpartum necrosis (Sheehan’s Syndrome) Pituitary tumors (most common cause) Aneurysms of intracranial carotid artery Thrombosis Infectious disease Ex – pyrogenic abscess, TB, syphilis Infiltrative disease Ex – hymosiderin, amylloid Immunologic (autoimmune) Iatrogenic (head/neck surgery – poor prognosis) Metabolic (especially renal failure, azotemia) Most Common Cause = Pituitary tumor A tumor may: Compress the gland within the sella Invade the gland (destroy it) Hemorrhage (pituitary apoplexy) Causes of Secondary Hypopituitarism: Destruction of the pituitary stalk Hypothalamic disease “Worst Case” Form = Panhypopituitarism = complete loss of pituitary function The clinical features develop within a matter of hours or days DEATH Often hard to recognize initially. Often presents as a dysfunction of the target tissue (ex – adrenals) Clinical Features: ACTH Deficiency TSH Deficiency LH and FSH Deficiency GH Deficiency Prolactin Deficiency ACTH Deficiency: Weakness Postural hypotension Malaise Dehydration Vomiting Nausea Hypothermia Loss of axillary hair Loss of pubic hair TSH Deficiency: Dry skin Pallor Mental slowing Bradycardia Hoarseness Constipation Reduced or absent menstruation LH and FSH Deficiency: Females: Amenorrhea, breast atrophy, dry skin Age, duration, and magnitude dependent Males: Reduced testicular size, loss of libido GH Deficiency: Kids: Total or partial impairment of growth Adults: There is a normal, age-related decline But – some adults do have the syndrome hyperlipidemia, osteoporosis (appear to be correctable) premature wrinkling and aging increased body fat Prolactin Deficiency: Results only in the absence of post-partum lactation General Features: Skin – decreased turgor and a waxy character (also a thinness) Periorbital wrinkling (“premature aging”) (effects on the skin) Mild anemia (normo/normo) This is refractory to other forms of treatment Mental slowing, apathy, delusions, paranoia, psychosis (not always easy to appreciate this in the elderly) Ex – Loss of the ability to do mental calculations and to concentrate Short-term memory loss Depression Diagnosis: Do a direct assay of individual hormone levels. This will show low to absent hormone concentrations. If it’s a mild or partial hypopituitarism, it may be hard to tell if the clinical features are due to a primary pituitary dysfunction or to a target organ of the pituitary’s hormones. Pituitary Reduced T4 Reduced TSH 2o Vs. Thyroid Reduced T4 Increased TSH 1o “Hypothyroid” NOTE: Expect 4 of these on Quiz 2 (to differentiate 1o, 2o, 3o forms) Hyperpituitarism: Very distinct Have subgroups of diseases (with names for the disorders) Except in cases of rare hormone-secreting tumors, hyperpituitarism usually involves overproduction of only a single hormone a single set of symptoms The response is less dose-dependent The clinical picture is usually distinct: 1o = a functional tumor produces a biologically active substance 2o = most often caused by altered feedback ex - hyperprolactinemia due to increased estrogen secreted during pregnancy OR an ovarian tumor ACTH hypersecretion in response to hypofunction of the adrenals Ex – Addison’s – bronze color due to 1o adrenal disease TSH hypersecretion in response to hypofunction of the thyroid 1o GH Hypersecretion: If it occurs prior to epiphyseal closure gigantism (due to the prolonged growth period due to the delayed epiphyseal closure) If it occurs after epiphyseal closure acromegaly (disproportional tissue/bone/cell growth) Acromegaly: Thickened skin Increased pigmentation Visceromegaly (large organs – spleen, etc) Carpal Tunnel Syndrome Thyroid enlargement Arthropathy Large hands/feet Increased head size ( larger hat size) Dx Criteria for GH Hypersecretion: Clinical signs and symptoms Elevated GH levels But not absolute – can be suppressed by hyperglycemia Normal: Increased glucose decreased GH Definitive: GH levels not suppressed by glucose 1o ACTH Hypersecretion: Cushing’s Disease 90% of these result from a functional tumor (ex – basophilic adenoma or bilateral hyperplasia) Clinical: Same as for adrenocortical adenoma Most common in 30-60 year-old women The disease causes a 2o hypercortisolism Syndrome: Hypercortisolism due to exogenous cortisol administration or an overproduction by the adrenals Cushing’s: Disease Increased cortisol Increased ACTH Clinical: Vs. Syndrome Increased cortisol Decreased ACTH Central obesity Abdominal fat Hypertension Amenorrhea Hirsutism Muscular atrophy Weight gain Osteoporosis and compression fractures Increased capillary fragility increased skin lesions Reduced wound healing Hyperglycemia Increased skin pigmentation __??__ Dx: Typical clinical findings Elevated plasma cortisol (in 50% of people) Elevated urinary free-cortisol (in 85-95% of people) (unbound cortisol) Plasma ACTH elevated or inappropriate for the cortisol levels Differential: Adrenal tumor Ectopic ACTH production Prolactin Hypersecretion: Pharmacologic agents CNS disorders Inflammation/infections Trauma Neoplasms Pituitary tumors Idiopathic Most common form of pituitary hyperfunction. Most often due to a functional adenoma of the pituitary. Present in at least 25% of infertile women. Females: Oligomenorrhea or amenorrhea Lactation Mild hirsutism Infertility Males: Impotence Decreased libido Lactation (heroin is also a powerful stimulator of this) Dx: Elevated prolactin levels 15 to 20 ng/ml to 10,000 ng/ml if < 200 ng/ml: if tumor: TEST: 25 to 30 questions Next Wednesday 1st hour, in the GYM almost never due to a tumor 5000-10,000 ng/ml