Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
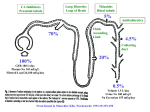
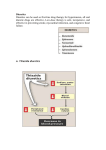
Diuretics Why do we want to know about diuretics? • • • • • What do kidneys do? What can go wrong? Interventions that can be used how do they work? Effects, side effects Functions of the kidney? • • • • Excretion of waste products regulation of salt and electrolyte content and volume of extra -cellular fluid acid -base balance How? • Several hundred litres of plasma filtered/day • filtrate - very little protein/protein bound substances • 99% of sodium is reabsorbed, some substances secreted • 1.5 litres voided as urine • Diuretics increase salt and water excretion Why diuretics? • important group of drugs employed for their effects on the kidney to enhance salt and water excretion (only when needed) • when used: heart failure, other causes of salt and water retention (renal failure, liver failure), hypertension Variety of compounds with diuretic activity • • • • • • • Xanthines - theophylline, caffeine osmotic diuretics - urea carbonic-anhydrase inhibitors thiazides loop diuretics aldosterone antagonists potassium sparing diuretics How do they work? • Direct effect on cells of the nephron.. • where most of the active and selective solute reabsorption occurs • ascending loop of Henle • early distal tubule • collecting tubules and ducts • OR • modifying the content of the filtrate by their presence Loop diuretics (Rang and Dale p361-363) • Frusemide, bumetanide, piretanide • act on thick segment of ascending loop • inhibit NaCl transport OUT of tubule by inhibiting Na+/K+/2Cl- carrier (co-transporter) in luminal membrane ( acting on chloride binding site) • Reduces the hypertonic interstitial area in the medull, so reducing water re-absorption • increases Na+ solute concentration in the distal tubule which is exchanged for K+ and H+ (hypokalemia and alkalosis) • Can increase the excreted sodium from 1% to 15% of filtrate • Also reduce peripheral vascular resistance Loop diuretics • Kinetics • • • • • oral and IV preparations bound to plasma protein, secreted into tubule metabolised by the liver ( P450) act within 1 hour half life about 90 minutes; longer in renal failure • duration - 3-6 hours (Lasts Six Hours – Lasix) Loop diuretics • Effects • pass urine – in large amounts! • Side effects • electrolyte depletion • Hypovolemia • other reactions rare • Main Use • • • • Heart failure – particularly acute left ventricular failure Hepatic cirrhosis Nephrotic syndrome Renal failure thiazide diuretics • bendrofluazide, hydrochlorothiazide, indapamide • act on distal convoluted tubule • bind to chloride site of Na+/Cl co–transport system and inhibit action • decrease active Na resorption • decrease water resorption • changes in Ca, magnesium and uric acid thiazide diuretcis • kinetics • rapidly absorbed orally • secreted into the tubule • maximal effect 4- 6 hours, duration 8-12 hours thiazide diuretics • effects • increase urine output • side effects • • • • electrolyte disturbances increased cholesterol impotence hypersensitivity reactions (rare) • Main uses • hypertension • mild heart failure aldosterone antagonists • spirololactone • inhibits action of aldosterone (intracellular receptor binding anatagonism), increases sodium and decreases potassium secretion • kinetics • well absorbed orally, active metabolite half life of 16 hours • effects • limited diuresis • Main uses – heart failure and cirrhosis • side effects • Hyperkalemia, estrogen like effects other potassium sparing diuretics • Triamterene, amiloride • act on collecting ducts • inhibit Na resorption, decrease potassium excretion • effects • limited diuresis • side effects • electrolyte disturbances clinical choices • Uses: • cardiac failure • hypertension • fluid overload • NOT for everyone with oedema (eg from venous insufficiency) • acute versus chronic • evidence of benefit references • Rang & Dale, 5th edition • Cardiovascular Therapeutic Guidelines • Australian Medicines Handbook


























![[4-20-14]](http://s1.studyres.com/store/data/006502231_1-6c6212a751ea6ee23ec20b8f55b90576-150x150.png)