Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacokinetics wikipedia , lookup
Psychopharmacology wikipedia , lookup
Discovery and development of direct Xa inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Spironolactone wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Neuropharmacology wikipedia , lookup
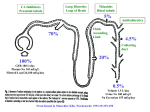
Pharmacology Lecture 7 Diuretics 1) Indicate the anatomical sites in the nephron where each class of diuretic drug acts. Osmotic Diuretics (red) – act in the proximal tubule and loop of Henle. Carbonic Anhydrase Inhibitors (blue) – act in the proximal tubule. Loop Diuretics (orange) – act in the thick ascending limb of the loop of Henle. Thiazide Diuretics (green) – act in the distal convoluted tubule. Potassium-Retaining Diuretics (purple) – act in the late distal tubule and collecting duct. 2) Describe the mechanism of action for each class of diuretic. Osmotic Diuretics – Mannitol is filtered by the glomerulus and not reabsorbed thus exerting an osmotic action. Na+ reabsoption is impaired in the proximal tubule and thick ascending limb. Carbonic Anhydrase Inhibitors – Acetazolamide inhibits the membrane-bound and cytoplasmic pools of carbonic anhydrase in the proximal tubule. Na+/H+ exchange normally causes Na+ to be pumped into the interstitium and H+ to react with HCO3- in the lumen to form H2CO3. Carbonic anhydrase converts this to CO2 and H2O. The CO2 diffuses into the epithelial cells where carbonic anhydrase converts it back to H2CO3. When this process is inhibited by acetazolamide, HCO3- is lost, resulting in metabolic acidosis and an increase in Na+ and Cl- delivered to the loop of Henle. Loop Diuretics – Furosemide (or ethacrynic acid) inhibits the Na+/K+/2Cl- symporter of the thick ascending loop of Henle. This causes an increase in Na+ and Cl- excretion with an associated increase in Ca2+ and Mg2+ excretion due to the loss of the electrochemical gradient that drives their transport. The Na+ that reaches the distal tubule causes increased K+ and H+ excretion. Thiazide Diuretics – hydrochlorothiazide (or thiazide-like chlorthalidone) inhibits Na+/Cl- symport in the distal convoluted tubule thus causing a moderate increase in Na+ and Cl- excretion, chronic uses decreases Ca2+ excretion. Potassium-Retaining Diuretics – Triamterene and ameloride inhibit epithelial Na+ channels of the late distal tubule and collecting duct where Na+ is exchanged with K+ and H+ thus causing slight NaCl excretion without K+ loss. Aldosterone antagonists – Spironolactone is a competitive antagonist of the high affinity aldosterone receptors found in the cytoplasm of the late distal tubule and collecting duct, which when activated, cause NaCl reabsorption with K+ and H+ secretion into the tubular lumen. Spironolactone block this action causing NaCl excretion without K+ loss, much like the potassium sparing diuretics. 3) Describe the use of the various types of diuretics in the management of edematous and non-edematous disorders. Diuretic Uses Mannitol Transient management of cerebral edema Promote renal excretion of toxins Maintenance of renal blood flow during vascular surgery Acetazolamide Glaucoma, Altitude sickness, Anti-seizure medication Rarely as diuretic Furosemide Pulmonary edema, Heart failure, Hypercalcemia *Loop diuretics are appropriate for edematous disorders in all but emergent situations Hydrochlorothiazide Antihypertension treatment, edema states, Ca+ nephrolithaisis, Osteoporosis, nephrogenic diabetes insipidous Triamterene & Not very efficacious, for use in combination with loop diuretics or Amiloride thiazides to offset their kaluretic effects Spironolactone Coadministration with other diuretics in the treatment of edema and hypertension, also beneficial in congestive heart failure 4) Describe the interactions of diuretics with digoxin, angiotensin converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs and sulfonamide drugs (antimicrobials, certain COX-2 inhibitors and oral hypoglycemics). Drug Interaction Digoxin Potassium-wasting diuretics (loop diuretics and thiazides) are contraindicated because they increase the likelihood of digoxin toxicity ACE inhibitors Potassium-retaining diuretics are contraindicated because they may cause hyperkalemia NSAIDs Blocks prostaglandin mediated renal blood flow Potassium-retaining diuretics are contraindicated Sulfonamides Furosemide should not be given to people with hypersensitivity to sulfonamides 5) Describe the pathogenesis of diuretic-induced to fluid and electrolyte imbalance. The major adverse effects of diuretics are fluid and electrolyte imbalance. Osmotic diuretics can cause an increase in intravascular volume thus causing or worsening heart failure. Carbonic anhydrase inhibitors cause metabolic acidosis. Loop diuretics can cause dehydration with increase in BUN and creatinine, hypo or hypernatremia, hypokalemia, and mild metabolic acidosis. Thiazides cause similar fluid and electrolyte imbalances to loop diuretics. Potassium sparing diuretics can cause hyperkalemia, which can be life threatening. Aldosterone antagonists can also cause hyperkalemia.