Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
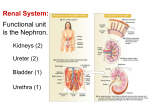
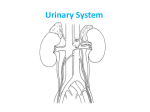
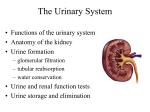
Ch. 23: The Urinary System Mat share anatomy with the reproductive system (males). Comprises urogenital system. Two kidneys, two ureters, bladder and urethra. I. Functions (A) Kidney Functions -1- eliminate wastes -2- regulate blood volume and pressure -3- regulate osmolarity of body fluids -4- secrete renin -5- secrete erythropoietin -6- regulate pH -7- calcitriol (vitamin D) synthesis -8- detoxify free radicals and drugs -9- gluconeogenesis (from amino acids) when necessary (B) Nitrogenous Wastes These are metabolically derived (from body chemistry). 50% urea (from protein catabolism), created from ammonia. Also uric acid (from nucleic acids) and creatinine (from CP). BUN = blood urea nitrogen, when too high leads to renal failure. (C) Excretion: done by four organ systems: -1- respiratory release of CO2 -2- integumentary, via sweat -3- digestive elimination -4- urinary release of metabolic wastes II. Kidney Anatomy (A) Gross Anatomy Kideney indented at hilum, attachment of vessels, nerves and ureter. Retroperitoneal location. Protected by fasciae, fat and renal capsule. Parenchyma (glandular tissue) envelopes sinus, contains medulla, cortex, pyramids, columns, papillae, minor and major calyces, pelvis (within sinus). 27 (B) Nephrons ~ 1.2 million/ kidney. -1- renal corpuscle: glomerulus (modified capillary bed) surrounded by Bowman’s Capsule, inner lining with podocytes. -2- renal tubule: ~ 3 cm long. a. proximal convoluted tubule = PCT. Simple cuboidal ET w/ microvilli (brush border). b.: Loop of Henle: descending and ascending limbs, thin and thick segments (squamous vs. cuboidal epithelium). c. DCT- also cuboidal walls. d. collecting duct: shared by several nephrons. Converge into papillary ducts, drain into minor calyces. -3- types of nephrons a. cortical – most. b. juxtamedullary – very long loops. Only ~ 15%. Maintain salinity gradient necessary for water conservation. -4- blood supply: kidneys receive ~ 20% of cardiac output. Renal artery -> interlobar a. -> arcuate a. -> interlobular a. -> afferent arterioles -> glomerulus -> efferent arteriole -> peritubular capillaries (around cortical nephrons) -> interlobular vein -> arcuate vein -> interlobar vein -> renal vein. Juxatglomerular apparatus between DCT and afferent arteriole. Renal medulla provided with vasa recta (instead of peritubular capillaries) surrounding juxtamedullary nephron loops. -5- nerve supply: renal nerves mostly sympathetic. III. Glomerular Filtration (A) Filtration Membrane: consists of three barriers -1- fenestrated endothelium of capillary, still excludes blood cells. -2- basement membrane: a proteoglycan gel. -3- filtration slits between extensions (pedicels) of podocytes. 28 Filtered blood components = water, electrolytes, glucose, fatty acids, amino acids, nitrogenous wastes and vitamins. Membrane damaged by trauma and infections, leads to proteinuria and hematuria. (B) Filtration Pressure: unique features -1- very high BP, partially due to afferent arteriole being wider than efferent. -2- high hydrostatic pressure in capsular space. -3- glomerular filtrate low in protein, no COP. Creates a positive net filtration pressure (NFP). (C) Glomerular Filtration Rate = GFR. 180 L/ day in men, 150 in women. (D) Regulation of GFR -1- renal autoregulation: a. myogenic mechanism – smooth muscle contracts when stretched. Stabilizes filtration even when afferent arteriole BP changes. b. tubuloglomerular feedback – JG cells in afferent arteriole, macula densa of DCT control diameter of afferent arteriole. -2- sympathetic control: reduces GFR, constricts afferent arteriole. -3- renin-angiotensin mechanism: when BP drops. JG cells secrete renin: angiotensinogen ->angiotensin I ->angiotensin II (active hormone) in lungs, requires ACE. Results in: a. vasoconstriction, increases BP. b. constricts afferent and efferent arterioles. c. stimulates ADH d. stimulates aldosterone e. stimulates thirst. IV. Tubular Reabsorption and Secretion > 99% of filtrate reabsorbed, 1-2L urine/ day. 29 (A) PCT ~65% of reabsorption, some secretion. Many mitochondria for active transport. Transcellular and paracellular (between cells) routes. Absorbed substances = Na+, Cl-, bicarbonate, other electrolytes, glucose, nitrogenous wastes (urea), water. Movement into peritubular capillaries. Transport maximum for most substances. Secretion: movement from capillaries into tubule. Drugs, toxins, bicarbonate, H+s. (B) Loop of Henle (nephron loop): for urine concentration. Some reabsorption of electrolytes and water. (C) DCT and Collecting Duct: subject to hormonal control -1- aldosterone: increases Na+ reabsorption. K+ secretion -2- ANP: increases GFR, inhibits aldosterone, renin, ADH, decreases NaCl reabsorption form collecting duct. -3- ADH: increases water permeability in collecting duct, increases water reabsorption. -4- PTH: increases Ca++ and MG+++ reabsorption, stimulates calcitriol synthesis. V. Water Conservation (A) Collecting Duct: extracellular fluid more hypertonic deeper in medulla, collecting duct becomes more permeable towards medulla. This concentrates urine. (B) Control of Water Loss: hormonal adjustments effect reabsorption to maintain body fluid and BP homeostasis. (C) Countercurrent Multiplier: salinity in medulla enhanced by fluid movement in opposite directions: descending, then ascending. Water leaves descending segment, promotes electrolyte reabsorption from ascending limb. Urea leaving collecting duct helps maintain high solute concentration in medulla. (D) Countercurrent Exchange with vasa recta: exchanges NaCl for water. Doesn’t interfere with steep salinity gradient in medulla. VI. Urine and Renal Function Tests Urinalysis is easy and informative. 30 (A) Composition and Properties of Urine -1- appearance: color due to urochrome, cloudiness due to WBCs, bacteria. -2- odor: ammonia from bacterial action. -3- specific gravity: concentration of solutes. -4- osmolarity: hypo- or hypertonic, depending on need. -5- pH: usually slightly acidic. Effected by diet. -6- chemical composition: average 95% water, 5% solutes (most abundant= urea). (B) Volume: polyuria (linked to diabetes), oliguria, anuria (< 100 ml/ day). Diuretics increase volume, either by increasing GF or decreasing reabsorption. Caffeine dilates afferent arteriole, increasing filtration. Alcohol suppresses ADH. (C) Renal Function Tests -1- renal clearance: volume of plasma cleared of waste/ min. e.g. normal for urea ~ 60 ml/ min. -2- GFR: measured with inulin (polysaccharide in some plants- not secreted or reabsorbed). GFR = clearance. Can be estimated with creatinine. VII. Urine Storage and Elimination (A) Ureters ~ 25 cm long. Urine moves peristaltically. (B) Bladder lined with detrusor muscle. Mucosa with rugae for expansion. Trigone on bladder floor suseptible to infection. Full at 500 ml, maximum ~700-800 ml. (C) Urethra: 3-4 cm in women, 18 cm in men: prostatic, membranous and spongy (penile) portions). Internal urethral sphincter from detrusor muscle, external sphincter near pelvic floor with skeletal muscle. (D) Voiding Urine = micturition. Detrusor muscle contraction parasympathetic. Regulated voluntarily via external sphincter, 31