Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
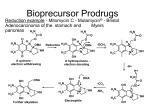
Hypoxia-activated prodrugs for cancer: conception to clinic Bill Denny Auckland Cancer Society Research Centre • Cancer is primarily a genetic disease; mutations in our DNA result in mutations in key proteins that control cell division • Every cancer’s genome has different combinations of DNA mutations, and thus a different suite of altered proteins Signalling networks in a cell But at the level of tissue physiology, virtually every cancer is different from all normal tissue – it’s hypoxic. Can we target this? Hypoxia in solid tumours • Functioning (cancer) cells need oxygen, so tumours need to develop their own blood supply to grow beyond a few millimetres in diameter • • • But they are very bad at it Thus tumour cells remote from blood vessels are hypoxic Long since recognised as a limitation of radiotherapy Necrotic Hypoxic Aerobic O2 Normal Tumour In 1986 we had an idea…………… Journal of Medicinal Chemistry ©Copyright 1986 by the American Chemical Society June 1986 Volume 29, Number 6 Perspective Considerations for the Design of Nitrophenyl Mustards as Agents with Selective Toxicity for Hypoxic Tumor Cells William A. Denny* and William R. Wilson* Cancer Research Laboratory and Section of Oncology, Department of Pathology, University of Auckland, School of Medicine, Private Bag, Auckland, New Zealand. Received. September 9, 1985 Windansea Beach, La Jolla, CA Bill Wilson Prodrugs with oxygen sensors • • A prodrug is defined as an inactive (non-toxic) compound, converted in the body to an active drug Activate by electron addition thru cellular reductase enzymes. Hypoxia prodrug design Hypoxia prodrug mechanism Importance of prodrug diffusion and bystander effect (cartoon) Non-toxic prodrug Activated drug Blood vessels Necrosis Hypoxic regions Cross-section through a human head-and-neck tumour What oxygen sensor? Oxygen sensor needs to: • be rapidly reduced by cellular reductases to a 1-electron adduct • adduct needs to be stable enough so that in oxygenated (normal) cells if can be reoxidised to the original prodrug • adduct needs to undergo further changes in hypoxic cells the that activate the toxin NITROBENZENES What toxin? Toxin needs to: • • • • be deactivated/activated by the oxygen sensor have a well-understood mechanism be a potent and ubiquitous cell killer (kill cells in a variety of proliferative states and pH environments) have good bystander effects NITROGEN MUSTARDS 8 Nitroaniline mustards as hypoxia prodrugs? • • Potency of “mustards” depends almost entirely on the electron density at the mustard nitrogen Nitro to amino change gives a large increase in electron density, resulting in an 10,000-fold increase in potency towards cells in culture R N Cl Cl 10,000fold Easy; is this our lead compound? 1985 1993 2004 Optimising biological properties: diffusion • 3D cell cell culture in a controlled atmosphere • Physics and mathematical modelling of diffusion kinetics • Can the prodrug reach remote hypoxic tumour cells? • Need fast diffusion and slow metabolism • Less water-soluble prodrugs diffuse more rapidly 100 Surviving Fraction 10-1 10-2 10-3 10-4 TPZ 10-5 10-6 10-7 10-8 5x increase in diffusion coefficient 10-9 10-10 0.01 0.1 1 10 Oxygen concentration (µM) A “pre-prodrug” concept to solve a dilemma • • • • • Dilemma: need lipophilic drug for good diffusion, but a watersoluble drug for iv injection. Increase aqueous solubility by converting alcohol to phosphate (PR-104) Rapid non-specific cleavage of this by phosphatase enzymes in serum to lipophilic alcohol PR-104A; rapid diffusion to hypoxic regions Activation by reductases to active amine PR-104M This stable enough to have a good bystander effect PR-104 PR-104A PR-104M Selection of lead candidate (2004) • Selected candidate PR104 from 6 final compounds (allday discussion) • Compromise between activity, potency, hypoxic selectivity, toxicity, ease of synthesis (cost of goods) PR-104 does preferentially kill hypoxic HT29 human colon cancer cells in model tumours HT29 human HT29 colonhuman carcinoma colon xenografts carcinoma xenografts Xenografts: single drug dose Single prodrug Single dose prodrug at MTD dose at MTD .999 99 • 99.9 99 90 Cell killing in human cervical cancer xenografts in immune-deficient mice An initial radiation dose kills all the oxygenated cells (about 95% of the tumour) • PR-104 kills up to 3 logs (99.9%) of the remaining radiotherapy radiotherapy Radiotherapy Radiotherapy Radiotherapy Radiotherapy hypoxic tumour cells + PR-104 29 TP Z 90 99.99 (20TP GyZ ) RASN D 292 +T 4 PZ4 RA DRA +D SN( 220 9G 24y 4) RA D +T PZ RA D +S N 29 24 4 9.9 99.999 24 4 9.99 Tumor cell kill (%) • (oxic cells) D RA SN (kills oxic (kills cells)oxic plus cells)PR-104 plus PR-104 (hypoxic cells) • In vivo proof-of-concept a major requirement So, are we done…….? To clinical trial: start-up company Proacta Inc • • • • Much of the 15 years of work (1986-2001), to this point was done under grants from the HRC of NZ, CR UK, and the US NCI: resulted in enough IP to set up a startup company In 1998, with UK ICR, set up EPTCO; could not raise UK funding In 2001, UniServices transferred assets to Proacta Therapeutics NZ; still took 3 years to raise $US 12M from Aust, NZ, Switzerland PR-104 first went to clinical trial in 2006 (Waikato, Auckland, US); then raised another US $35M from US; Proacta Inc in San Diego Trevor Twose CEO 1998-2000 Aki von Roy CEO 2000-2004 Paul Cossum CEO 2004-2006 John Gutheil CEO 2006-2012 PR-104: Discovery/development timeline date task 1986-2001 Development of concept and methods discovery 2003 Nine advanced phosphate pre-prodrug candidates 2001-2004 Set-up and funding of Proacta development 2004 PR-104 selected by Proacta to develop 2005 GMP scale-up, drug formulation decided, animal safety toxicology completed, IND submitted to FDA and approved Jan 2006 First patient treated at Waikato Hospital May 2007 Phase I completed 2008 Phase II trial in non-small-cell lung cancer But then, the unexpected (which you should always expect!). Activity in Phase II in NSCLC and leukemia, but variable toxicity Also see aerobic activation of PR-104 in some human cancer cell xenografts 70 H460 NSCLC Low % of hypoxic cells A1 Percentage hypoxic* cells 60 50 40 % of hypoxic cells in various cancer xenografts 30 E2 20 B3 10 0 H460 C33A SiHa HT29 22Rv1 A549 HCT116 A2780 250 In vitro PR-104A aerobic reduction 200 Extent of aerobic metabolism of PR-104 pmol PR-104H+M /106 cells 100 80 60 40 20 Control C33A A2780 HCT116 H1299 MDA231 MiaPaCa PC3 22RV1 HT29 SiHa H460 A549 0 H1299 A new aerobic nitroreductase (AKR1C3) AKR1 cluster • Microarray profiles of genes in 23 human tumour cell lines show high aerobic toxicity to PR-104 correlates with expression of AKR1C3, a member of the aldoketo reductase (AKR) gene family (not known as a nitroreductase). • Only AKR1C3 reduces PR-104 under aerobic conditions. • AKR1C3 reduces only PR-104 under aerobic conditions (not even the class A and D series) B A 160 40 20 V5 TAG NQO1 AKR1B10 AKR1B1 AKR1C3 AKR1C2 AKR1C1 WT 0 C33A A2780 H1299 HCT116 MiaPaca 2 MDA231 8 22Rv1 PC3 60 10 SiHa HT29 80 12 H460 100 14 HCT116 AKR1C3 #1 HCT116 AKR1C3 #3 A549 120 IC50 ratio (WT/AKR1C3) 16 HCT116 AKR1C3 PR-104M PR-104H 140 No V5 induction control pmol PR-104A metabolites formed per 106 cells 18 AKR1C3 6 Actin 4 2 0 4 9 e 9 A C N in le le zo azo -106 195 crin -104 Q4 cin myc EO a A a y B d d r U C t ro ni ni PR Ni tom rfi RS so tro Mi Po Mi Me AKR1C3 18 C Where now for PR-104? • A Phase II trial in leukemia showed about 30% responses, but still unpredictable aerobic activation so Proacta terminated their development of it in 2012. • Plans are underway for a new (noncommercial) trial by the US Southwest Oncology Group in relapsed T-cell lymphoblastic leukemia, which overexpresses AKR1C3 (exploiting this weakness). We are supplying the clinically formulated drug Hypoxia-activated prodrugs that didn’t make it Despite a compelling biochemical rationale and much work by many, no hypoxia-activated prodrug has yet been FDA- or EMA-approved Where now for hypoxia-activated prodrugs? Apart from PR-104 we also have: − Tarloxotinib, a completely different class, now in Phase II trials in NCSLC in the US − an A-series AKR1C3proof analogue of PR-104 about to be trialled in Europe − a lead candidate in a third new class; looking for a commercial partner Conclusions • • • No hypoxia-activated prodrugs yet registered; a quixotic quest? No, this is where academic involvement in drug discovery should be; longer time horizon; can be more innovative (note half of all classes of current cancer drug had their origins in academic groups) This project could not have been started in a large pharma: – – • • • concept not “validated”, thus much too risky PR-104 has nitro groups, a mesylate and a halide; all on the “toxic” list of no-no substituents) Drug development in a new field can take a long time; need to develop analytical methods to measure (e.g.) drug diffusion through tissue, reductive enzymology, hypoxia biomarkers In hindsight, we made the wrong initial choice of sub-class to develop with PR-104 (AKR1C3 susceptibility of class B) but could not know that Tarloxotinib may be the “breakthrough” compound in the field? ASCRC staff Commercial and grant sources