Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Acute respiratory distress syndrome wikipedia , lookup
Cardiac output wikipedia , lookup
High-altitude adaptation in humans wikipedia , lookup
Alveolar macrophage wikipedia , lookup
Intracranial pressure wikipedia , lookup
Homeostasis wikipedia , lookup
Physiology of decompression wikipedia , lookup
Hemodynamics wikipedia , lookup
Biofluid dynamics wikipedia , lookup
Circulatory system wikipedia , lookup
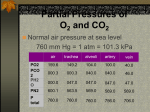
BHS116 Fall: Human Physiology and Pathology Notetaker: Jessica Du Date: 10/05/2011, 1st hour Page1 Transport of O2 and CO2 in blood to and from cells Respiration: - Goal is to provide oxygen to the tissues and to remove carbon dioxide - Four major functions o 1. Pulmonary ventilation (air lungs) o 2. Diffusion of O2 and CO2 between alveoli and blood o 3. Transport of O2 and CO2 in blood to and from cells Focus on this! o 4. Regulation of ventilation Gas Transported in Blood: - The amount physically dissolved is directly proportional to the partial pressure - [amt gas dissolved] ∝ Pgas - The main difference between the transport of O2 and CO2 is that CO2 has a higher solubility coefficient o Higher solubility coefficient Higher [gas] dissolved High partial pressure - Dissolved O2 is too low to supply the tissues o Only 15 mL/min, tissues at rest requires 250 mL/min of O2 Hemoglobin binds up the O2 and carries it to the tissues Hb allows for 30-100 times more O2 transport and 15-20 times more CO2 transport Hemoglobin: - 2 α peptides - 2 β peptides - Each chain contains a heme group with an iron atom - The iron atom binds 1 O2 molecules - A total of 4 O2 can bind a single Hb protein (fully saturated) Transport of O2 in Blood: - The % saturation of hemoglobin is directly related to the PO2 of the blood - Hb binding with O2 is reversible o Increased PO2 increases Hb saturation (Hb associate more with O2) o Decreased PO2 decreases Hb saturation (Hb dissociates more O2) - When alveolar PO2 = Blood PO2 (no Hb) no diffusion - When alveolar PO2 > Blood PO2 O2 binds Hb o Since have O2 bind, now can deliver more O2 systemically - When alveolar PO = Blood PO2 (saturated Hb) decreased O2 binding to Hb Oxygen-Hemoglobin Dissociation Curve: - 100% saturation: 15 g of Hb/100 mL = 20.1 mL of O2/100 mL of blood - Arterial blood is at 98% saturation = 19.7 mL O2/100 mL of blood o Pulmonary capillaries High PO2 High Hb-O2 association - Venous blood is at 75% saturation = 14.4 mL O2/100 mL of blood o Systemic capillaries Low PO2 High Hb-O2 dissociation o 19.7 – 14.4 ~ 5 mL = the amt of O2 delivered per 100 mL of blood Note: when PO2 < 40 mmHg, very steep Hb-O2 release - 98% of blood entering the left atria from the ling has passed through the alveolar capillaries o 2% is shunted from the aorta-bronchial circulation-pulmonary veins-left atria and is “not oxygentated” This is referred to as the pulmonary shunt blood There is blood flow there, but very little exchange occurs BHS116 Fall: Human Physiology and Pathology Notetaker: Jessica Du Date: 10/05/2011, 1st hour Page2 Diffusion of O2 from Capillaries into Tissues: - O2 is constantly being consumed by cells. Thus PO2 is low in tissues resulting in the influx O2 o Diffusion gradient: PO2 in artery =100 mmHg > PO2 in tissue = 40mmHg O2 flows down its concentration gradient, and results in the delivery of O2 to tissues During Changes in Atmospheric Oxygen: 1) Ascending a mounding o Alveolar PO2 decreases from 100 mmHg 60 mmHg o ∆PO2 is 40 mmHg, results in 8% less saturation of Hb than normal o Venous PO2 decreases from 40 mmHg 35 mmHg o ∆PO2 is 5 mmHg, saturation is relatively the same - Still would get 5 mL of O2 deliverer to tissues per 100 mL of blood - A decrease in alveolar PO2 (40 mmHg) only resulted in a 5 mmHg decreased in the tissue PO2 .`. while climbing a mountain, tissue delivery of O2 is relatively unchanged, despite the changes in the starting alveolar pressure 2) Diving below sea-level - If you increase PO2 to 500 mmHg o Max PO2 can only go potentially 2% higher (it was 98% saturated to begin with) .`. not really increasing the amount of O2 bound to Hb very much o After loss of 5 volumes percent by release to the tissues, PO2 is only 2-3 mmHg greater than normal ∆PO2 in tissue = 43 – 40 = 3 mmHg Hemoglobin Buffers Tissue PO2: - Upper limit is ~40 mmHg (normal conditions) o If tissue PO2 was higher, PO2 would not leave Hb - Lower limit is ~ 15-20 mmHg (exercise) o Small decrease in PO2, and big increase in O2 released (due to the steep part of the Hb-O dissociation curve) Hb-O2 Dissociation Curve Shifts: - 1) Bohr Effect: Right of Left shift in the curve in response to change circulation levels of: o 1. PCO2 o 2. H+ (pH) Right Shift: Tissue capillaries ↑ PCO2 ↑ H2CO3 ↑ H+ ↓ pH .`. ↓ O2 Binding Left Shift: Pulmonary capillaries ↓ PCO2 ↓ H2CO3 ↓ H+ ↑ pH .`. ↑ O2 Binding We do not see this often in normal cellular activity Could see this at alveolar level, during the recovery from a right shift back to normal dissociation curve - Note that the binding of O2 and CO2 to Hb affect the binding of each other - 2) BPG (2,3-biphosphoglycerate) Effect o BPG is synthesized in RBC in hypoxic events (eg: when climbing a mountain) o During hypoxia, BPG may shift the dissociation curve to the right as much as 10 mmHg Increases O2 delivery (increase PO2, increase dissociation) Because during hypoxia, you need to increase as much O2 release as possible o Important adaptation during poor tissue blood flow BHS116 Fall: Human Physiology and Pathology Notetaker: Jessica Du - - Date: 10/05/2011, 1st hour Page3 3) Temperature Effect o Increase in temperature also result in a shift to the right Increased O2 dissociation from Hb Important during times to illness when fever is present Want to increase O2 delivery to tissues, so lymphocytes and macrophages receive enough O2 to function and fight off infection 4) Exercise Effect o ↓ pH (due to lactic acid build up) o ↑ pCO2 (at tissue) o ↑ temperature (due to ATP used during muscle contraction) o Results in a right shift of the dissociate curve, resulting in an increase in O2 delivery CO2 Transport: - Remember that CO2 is 20x more soluble than O2 in water (blood), due to its higher solubility coefficient - Carbonic anhydrase is an enzyme which catalyzes conversion of CO2 and H2O H2CO3 which dissociates into H+ and HCO3o This occurs 5000x times faster in cell vs plasma, due to the presence of the enzyme o CO2 is transported at the greatest percentage as HCO3- in the blood (60%) - - HCO3-/Cl- cotransporter (antiporter): found in both tissue RBCs and alveolar RBCs Results in a Cl- shift between venous and arterial blood RBCs At tissue: o PCO2tissue > PCO2blood causes the diffusion of CO2 into the blood o This CO2 will combine with Hb, which knocks off some O2, so it can participate in gas exchange at the tissue o CO2 also enters the RBC CO2 + H2O H2CO3 H+ + HCO Increase H+, which also is able to combin with Hb, and knock off more O2 for tissue O2 delivery At alveoli o PCO2 blood > PCO2 alveoli cause diffusion of CO2 into alveoli o Changes in HCO-/Cl- cotransporter, HCO3- in and Cl- out BHS116 Fall: Human Physiology and Pathology Notetaker: Jessica Du Date: 10/05/2011, 1st hour Page4 Diffusion of CO2 from the tissues into the capillaries (tissue PCO2 = 46, blood PCO2 = 40) - CO2 diffuses in the opposite direction of O2 - CO2 diffuses 20x faster than O2 CO2 dissociation curve - Very narrow range, of only 40-46 mmHg results in 4% of total CO2 being released into alveoli o Small change in PCO2, relatively high delivery o Due to high solubility coefficient of CO2 Haldane Effect - Decreased O2 binding to Hb increased CO2 and H+ binding to Hb (at tissue capillaries) - Opposite of Bohr effect - ** don’t need to know graph for exam Carbon Monoxide Binding - Hb has a very high affinity for CO, than O2 o Extremely low PCO can bind Hb easily, due to its higher affinity than O2 o PCO = 0.4 mmHg is enough to complete equally than O2 o PCO = 0.6 mmHg is enough to out compete O2 and cause CO poisoning