Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
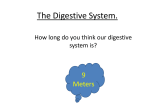
Upper Gastrointestinal Cancers Top ⑩ Tips GLOUCESTERSHIRE CANCER SUMMIT WEDNESDAY 30TH SEPTEMBER 2015 MR SIMON M HIGGS CONSULTANT UPPER GI SURGEON THREE COUNTIES OESOPHAGOGASTRIC CANCER UNIT, GLOUCESTER ROYAL HOSPITAL The Bottom Line! Oesophagus 8300 Stomach 7100 Pancreas 8800 Are they preventable? 89% of Oesophageal, 75% of Stomach and 37% of Pancreatic Cancers are linked to preventable/treatable lifestyle and other risk factors = ~16000 cancers Back in the real world! Prevention is the goal How can we improve outcomes Improve patient awareness Optimise 2 week wait referral pathways Reduce emergency presentations Increase capacity in secondary care Better access to diagnostic tests TOP ⑩ TIPS OESOPHAGO-GASTRIC PANCREATIC ①&② ANAEMIA ⑧ ULTRASOUND ③ DYSPHAGIA ⑨ CA 19.9 ④ ENDOSCOPY ⑤ EARLY CANCERS ⑥ FAMILY HISTORY ⑦ BARRETT’S OESOPHAGUS GENERAL ⑩ DYSPEPSIA AND WEIGHT LOSS, RECURRENT DYSPEPSIA/REFLUX, PROLONGED PPI TREATMENT ①② Anaemia Non-Iron deficient anaemia (Low Hb, Normal MCV/Ferritin) alone is associated with a very low pick up rate of oesophageal or gastric malignancy Iron deficiency anaemia (IDA ie. Low Hb, Low MCV+/-Ferritin ) without specific upper GI symptoms should be investigated via an IDA 2WW Pathway Causes of IDA Aspirin/NSAID use 10-15% Colonic Carcinoma 5-10% Gastric Carcinoma 5% Oesophageal carcinoma 1-2% ③ Dysphagia Food getting stuck on swallowing has the highest positive predictive value for the identification of OG cancers BUT: Only present in 40% of patients with oesophago-gastric cancers Is often a sign of more advanced disease AND: Should always be referred urgently for endoscopy ④ Endoscopy v Barium swallow OGD is the investigation of choice for upper GI symptoms More information Instant Safe Biopsy options Barium swallow is not an easy option even in the very frail and any abnormality will need an endoscopy to confirm ⑤ The earlier the better Oesophageal Cancer Gastric Cancer Pancreatic Cancer ⑥ Family History Stomach cancer risk is 2-10 times higher in people with a family history of the disease 1-3% of stomach cancers are linked to inherited stomach cancer predisposition syndromes (eg hereditary non-polyposis colon cancer (HNPCC)) Stomach cancer risk is higher in people with BRCA2 mutation in their family ⑦ Barrett’s Oesophagus Barrett’s oesophagus significantly increases the risk of oesophageal cancer Barrett’s with no dysplasia = 0.25% risk per year Barrett’s with high grade dysplasia = 6% Increased risk with Untreated GORD, smoking, male sex, advancing age and obesity Key Interventions: Treat GORD – PPI or Anti-reflux surgery 2 Yearly surveillance with biopsy Early referral for change in symptoms ⑧ Jaundice and Ultrasound Patients with jaundice should have an abdominal ultrasound and LFTs before referral to 2WW pathway Differentiate other causes of jaundice (ie non-obstructive) Next management clearer with US result Earlier specialist referral Gallbladder stones and dilated duct – MRCP and/or ERCP No Stones and dilated duct – CT and ERCP/PTC ⑨ CA 19-9 The tumour marker CA 19-9 is not recommended as a screening test Seen in benign conditions, such as the following: Biliary tract obstruction Cholangitis Inflammatory bowel disease Acute or chronic pancreatitis Liver cirrhosis Cystic fibrosis Thyroid disease 5% of the population do not produce CA 19-9 Test in the presence of a proven pancreatic or biliary lesion or metastatic disease of unknown primary ⑩ Dyspepsia and other red flags Urgent 2WW referral should be considered for patients with: Persistent abdominal pain with weight loss Reflux symptoms requiring PPI for more than 5 years New onset of dyspepsia/reflux which recurs after stopping PPI (>55yrs) Any Questions?