Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
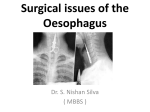
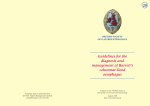
Barrett’s Oesophagus Dr Simon Moodie Barrett's oesophagus (Barrett's) is an abnormal lining of the oesophagus (otherwise known as the gullet), which occurs in patients with a long history of heartburn and reflux (acid and bile moving into the gullet). In a minority of people, Barrett's oesophagus may progress through a series of stages (dysplasia) to cancer. It is likely you have had reflux of stomach juices (acid, bile, enzymes) into your lower oesophagus for some time. This may have caused symptoms such as heartburn or indigestion. There will have been on going inflammation in your lower oesophagus because of your reflux and your body has “coped” with this by changing the nature of the cells that line the lower oesophagus. These have changed from the acid sensitive oesophageal cells to intestine type cells. This area of intestinal type cells is seen on the pictures below. This is called Barrett’s oesophagus. Barrett’s oesophagus is a risk factor for developing oesophageal cancer. How common is Barrett’s oesophagus? Studies suggest that a 1cm or more Barrett’s segment occurs in: Aproximately 8% of UK and USA adult population undergoing endoscopy. Aproximately 3% of UK and USA adult population. What is the risk of oesophageal cancer in Barrett’s? Risk is a hard thing to describe in a way that gives a reasonable perspective –here are the numbers from a recent (2016) review: annual risk of cancer for long (>3cm), short (1-3cm) and ultrashort (<1cm) Barrett’s segments are 0.22%, 0.03%, 0.01% respectively. This means if in one year 3440 patients with short segment Barrett’s have a surveillance endoscopy we would expect to find just one cancer. This is a very low risk indeed. The figure would be 450 for long segment Barrett’s. To put it another way, the risk of cancer is less than one in 400 a year for long segment and less than 1 in 3000 per year for short segment, less than 1 in 12,000 per year for ultrashort segment. How can the risk of cancer be lowered? Regular surveillance endoscopies probably lower the risk of dying from cancer by enabling your doctor to both diagnose pre-cancerous changes developing and also to diagnose very early cancers developing before they have caused any symptoms. This allows a better chance of the cancer being curable by surgery plus possible chemotherapy or radiotherapy. If precancerous changes are picked up at an endoscopy this may be “low grade dysplasia” or “high grade dysplasia”. Low grade dysplasia can sometimes be treated with ablation therapy to cauterize the whole segment of Barrett’s and allow more normal oesophageal cells to grow back. This treatment is relatively new, it can reduce risk of oesophageal cancer and is available on the NHS (via referral to specialist centres). High grade dysplasia is such a high risk that sometimes we suggest surgery (ranging from removal of small patches at endoscopy to major surgery to remove segment of oesophagus) What is the treatment of barrett’s oesophagus? Most patients have associated symptoms of reflux disease and/or oesophagitis (inflammation of the oesophagus) found at endoscopy. These patients clearly need long term treatment with drugs to lower acid levels (usually a proton pump inhibitor such as omeprazole or lansoprazole). This will not only improve symptoms but it is thought that it may reduce oesophageal cancer risk although this has not been conclusively proven. In patients with no symptoms and no oesophageal inflammation most gastroenterologists also recommend long term proton pump inhibitor treatment on the assumption that this will lower cancer risk, but again this is not completely proven and it is reasonable in this group of patients to sometimes be on no regular treatment if the patient has difficulty with the medication. What tablets can I not take? If you are on low dose aspirin, there is no reason to stop this unless you have had ulcers or bleeding into your gut. Indeed, it is possible that aspirin may help in Barrett’s but we do not yet know. Some medication may worsen reflux such as calcium antagonists (diltiazem, amlodipine) and some other drugs for high blood pressure and angina, also some oeteoporosis once a week drugs. It will be a question of weighing up the benefits of these drugs with the risks. Can I have an operation to treat my Barrett’s? No. There are anti-reflux operations available for gastro-oesophageal reflux disease to tighten the lower oesophageal sphincter. These are successful in some patients in reducing their need for long term medication for their reflux. Anti-reflux operations will not treat the Barrett’s but a few patients may opt for surgery to treat reflux symptoms. There is at present no convincing evidence that these operations can reduce risk of dysplasia or cancer in Barrett’s oesophagus. Endoscopic ablation can reduce cancer risk in low and high grade dysplasia (see above). In high grade dysplasia more radical surgery to remove the lower oesophagus is sometimes recommended. Summary The vast majority of people with Barrett’s oesophagus will never develop oesophageal cancer, but they are at a greater risk than the general population. We currently recommend intermittent endoscopies and regular acid suppressing drugs for most patients.