Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
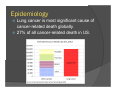
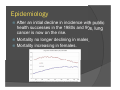
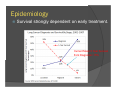
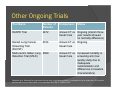
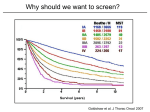
Lung Cancer Screening: An Evidence-Based Overview Sean A. Kennedy MD Ravi Shergill BSc Mark O. Baerlocher MD, FRCPC McMaster University, Hamilton, ON Royal Victoria Hospital, Barrie, ON All three authors have no conflicts of interest to declare. Learning Objectives Review the epidemiology of lung cancer. 2. Review the principles of screening programs. 3. Review the latest evidence for and against lung cancer CT screening, including the National Lung Screening Trial and other ongoing trials. 4. Review associated risks, limitations and implementation challenges of lung cancer screening. 1. Epidemiology Lung cancer is most significant cause of cancer-related death globally. 27% of all cancer-related death in US. Epidemiology After an initial decline in incidence with public health successes in the 1980s and 90s, lung cancer is now on the rise. Mortality no longer declining in males. Mortality increasing in females. Epidemiology Survival strongly dependent on early treatment. Current Mean 5 Year Survival from Diagnosis= 15% Mean “Principles and Practice of Screening for Disease” (WHO, 1968) In order for a screening program to be acceptable it must address a: Significant public health issue Treatable disease with defined practices on who to treat Disease with a latent stage where treatment can change outcomes and the progression is understood Disease that can be tested for Additionally, testing must be: Acceptable (ie non/minimally invasive) Economically sensible Continuous, ongoing process Past Screening Programs Chest X-ray (1-3x per year) Sputum cytology Combined cytology chest X-ray and sputum Past Screening Programs Systematic review of 9 trials (8 RCTs) with 453 965 subjects looked at whether sputum cytology, CXR or CT screening affects lung cancer mortality. No significant mortality reduction when screening with chest x-ray and sputum cytology was compared with chest x-ray alone (RR 0.88, 95% CI:0.74-1.03). PLCO trial annual CXR vs no CXR for 4 years (>150 000 participants, age 55-74, general population). No significant mortality reduction. (RR 1.05, 95% CI, 0.98-1.12). Conclusion: CXR and/or sputum cytology NOT recommended for screening. Manser et al Screening for lung cancer. Cochrane Review June 21 2013. National Lung Screening Trial NLST enrolled a high risk population of 53 454 current and former smokers. Inclusion criteria: Age 55 to 74 >30 pack year history of smoking Current smoker or quit within past 15 years Participants were randomized to annual screening with either low-dose helical CT or single-view chest radiograph for three years. National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395 NLST Definition of Positive Findings For low-dose CT: All non-calcified nodules with diameters >4 mm. For CXR: All non-calcified nodules and masses. Radiologist overall opinion (ie hilar adenopathy, pleural disease). National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395 C (A) CT image showing ground-glass RUL nodule. (B) 20 month followup progression to increasingly solid tumor. (C) Adenocarcinoma on biopsy. Source: MassGen Radiology Rounds Vol 4 Issue 8, Aug 2006 NLST Results The study was stopped early at a mean follow-up time of 6.5 years. Lung cancer mortality: CT arm 247 per 100 000 person-years CXR arm 309 per 100 000 person years Relative mortality benefit of 20.0% (95% CI, 6.8 to 26.7; P=0.004). National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395 Ongoing Trials NELSON Trial Dutch Belgian randomised lung cancer screening trial (NELSON). Only ongoing trial with sufficient power to detect mortality differences (n=15 822). RCT with population similar to NLST. Control arm receives usual care (ie no CXR). Intervention arm receives CT screen every 1,2 or 2.5 years. NELSON Trial Registration http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=636 Other Ongoing Trials Trial Name Number of Patients Comparison DANTE Trial 2472 Annual CT vs Ongoing (interim three Usual Care year results showed no mortality difference) Danish Lung Cancer Screening Trial (DLCST) 4104 Annual CT vs Ongoing Usual Care Multi-centric Italian Lung 4099 Detection Trial (MILD) Status Annual CT vs Increased mortality in Usual Care screening arm (low quality study due to inadequate randomization and differences in baseline characteristics) Humphrey et al. Screening for lung cancer with low-dose computed tomography: a systematic review to update the US Preventive services task force recommendation. Ann Intern Med. 2013 Sep 17;159(6):411-20. Other Ongoing Trials A large pooled analysis of UKLS, NELSON, MILD, DLCST, ITALUNG, LUSI and DANTE is planned for 2015/16. NELSON Trial Registration http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=636 Risks and Concerns Reproducibility Academic vs community The NLST involved primarily academic centres with fellowship trained thoracic radiologists reading the screening CTs. Unknown if applicable on large scale in community hospitals with general radiologists. Gill et al. Controversies in Lung Cancer Screening. J Am Coll Radiol 2013;10:931-936. False Positives False positives (20% after first screening CT, 30% after second). 7% of these false positives lead to need for percutaneous, thoracoscopic, open biopsies. Significant anxiety associated with false positives in other screening programs (not yet demonstrated for lung cancer screening). Croswell JM et al. Cumulative incidence of false-positive test results in lung cancer screening: a randomized trial. Ann Intern Med. 2010 Apr 20;152(8):505-12. Broderson et al. Long Term Psychosocial Consequences of False-Positive Screening Mammography. Ann Fam Med Mar/Apr 2013 Vol 11 no 2; 106-115. Radiation Dose Continued advances in dose reduction allow for minimal radiation exposure (~1.5 mSv per screening CT). Potentially >20 years of annual chest CT Unclear potential risk for radiationinduced cancer. Baerlocher et al. Discussing radiation risks associated with CT scans with patients. JAMA. 2010 Nov 17;304(19):2170-1. American College of Radiology and Radiological Society of North America (April 2012). Patient Safety: Radiation Dose in X-Ray and CT Exams . Retrieved March 23, 2015. Cost Efficacy No studies yet evaluate cost effectiveness in Canada’s public health care system. Studies in US forecast screening will be cost effective at <$19 000 (USD) per lifeyear saved. By comparison: Biennial breast screening costs $18 999 (USD) per life-year saved Colon cancer screening costs $11 900 (USD) per life-year saved Gill et al. Controversies in Lung Cancer Screening. J Am Coll Radiol 2013;10:931-936. Pyenson et al. Offering lung cancer screening to high-risk medicare beneficiaries saves lives and is cost-effective: an actuarial analysis. Am Health Drug Benefits. 2014 Aug;7(5):272-82. Propagation of Smoking? Some concerns whether effective screening and negative test results could paradoxically reassure smokers, reducing smoking cessation rate. However, an analysis of current smokers in NELSON found screening had no impact on quit rate. Van Der Aalst et al. The impact of a lung cancer computer tomography screening result on smoking abstinence. Eur Respir J. 2011 Jun;37(6):1466-73. Organizations Endorsing CT Lung Screening American Cancer Society American College of Chest Physicians American Society of Clinical Oncology National Cancer Institute US Preventive Services Task Force CancerCare Ontario Roberts H et al. Screening High-Risk Populations for Lung Cancer: Guideline Recommendations. Journal of Thoracic Oncology: October 2013;8(10):1232-1237. Conclusion Lung cancer screening holds great promise in improving lung cancer mortality. Numerous ongoing trials should help to clarify the role of screening for lung cancer. It remains to be seen if and how such a program will be implemented in the Canadian setting on a provincial or national level.