Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
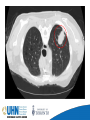
AN ONCOLOGY PATIENT’S JOURNEY… A PA’S PERSPECTIVE October 23, 2015 Maitry Patel, CCPA Physician Assistant Meredith Giuliani, MBBS, MEd, FRCPC Staff Radiation Oncologist Radiation Medicine Program Princess Margaret Cancer Centre Toronto, Ontario Disclosures • We have no potential conflicts with this presentation • We have no relevant financial relationships to disclose • We will discuss both generic and brand name medications • We will not be discussing any off-label medications Objectives • Define cancer, both in medical and layman’s terms • Explain the pathways for cancer management • Bridge gap between specialty services and community care, and explain oncology patient’s referral process from primary care to hospital setting • Explore the patient’s perspective • Demonstrate the role of PAs in a patient’s cancer journey • Review oncology patient’s survivorship and palliative goals What is cancer? • Oxford Dictionary definition of CANCER: A disease caused by an uncontrolled division of abnormal cells in a part of the body. • Definition of ONCOLOGY: The study and treatment of tumours. Characteristics of cancer 1. Uncontrolled growth of the cells in the human body 2. Ability of these cells to migrate from the original site and spread to distant site 3. Cancer is not a single disease But what goes through a patient’s mind? Discussion • What experiences have you had with patients’ new diagnoses of malignancies? • What kind of questions do they usually have? • What works when communicating with these patients? What doesn’t? A Day in Life of Maitry Outpatient Clinical: • New consults, follow-up, and on-treatment patients [history and physical, assessment and planning, breaking bad news, patient education, and obtaining patient consent] • Refer to specialty services Inpatient Clinical: • Monitor bloodwork; order and interpret imaging; manage post-op complications • Discharge summaries, daily rounds Patient Education: • Diagnosis, treatment modalities (surgery, radiation, chemotherapy, or a combination of two or more concurrently or in various orders) • Survivorship post being disease-free • Referral to palliative care/hospice Preceptorship and Education: • UofT and McMaster PA students and observers • Medical students during their elective rotation • Help orient new residents and fellows Research: • Recruit patients for ongoing clinical trials and monitor patients currently enrolled in trials • Serve as principal or co-investigator in identifying new therapies or developing techniques that help patients cope with the symptoms they experience from cancer or cancer treatment CME/Self-Study: • Tumor boards, grand rounds, resident half-day • Keep up-to-date with publications Administrative: • Call patients back regarding bloodwork and/or imaging results • Return patient and family calls, emails, etc. re: queries and concerns • Monthly PA Council meetings Surgical: • Mark and prep the patient, perform OR timeout • First assist, in addition to skin closure/dressings • Post-op orders, and handover to PACU nurses Discussion • What is your understanding of the existing cancer care pathway in Ontario? • What are your own experiences regarding navigating your patients through this? • What works well? What doesn’t work well? Existing cancer care pathway Prevention Screening Ontario Breast Screening Program: • Age 50-74: mammogram every two years • Age 30-69: referral for yearly mammogram and breast MRI at OBSP screening for Women at High Risk Ontario Cervical Screening Program: • Women who are or have been sexually active have a Pap test every 3 years starting at age 21 Colon Cancer Check: • All individuals aged 50 to 74 years with no family history of colorectal cancer should be screened every two years with FOBT • Individuals with first-degree relative with a history of colorectal cancer: colonoscopy beginning at age 50 Prostate Cancer: • No current screening guidelines • Avoid PSA testing in men with little to gain: Men 70 years of age and older Men with ≤ 10-15 year life expectancy Skin Cancer: • No current screening guidelines for general healthy population • High risk individuals: yearly physical exam Lung Cancer: Lung Lung Lung cancers cancers cancers detected detected detected Scan 1 Scan 2 Scan 3 270 168 211 Lung cancer deaths Total deaths 427 1877 503 1998 CT Total: 649 136 65 78 CXR Total: 279 Lung cancer deaths avoided 1 for every 320 people screened Discussion • About screening and prevention • What are some setbacks in current prevention and screening methods? • What can we do to increase screening and prevention rates in Ontario? Role of ER and GIM Let’s get to know Susan • 48 year old ♀ • PMHx: gastric ulcers, multiple endoscopies Meds: None on a regular basis || NKDA • FHx: mother: gastric ca, father: colorectal ca, brother: prostate ca, son: spinal muscular atrophy, daughter: retinoblastoma • SHx: Lifetime nonsmoker. Socially consumes EtOH. Works in social services How did she end up at PMH? • Initial presentation: L throat discomfort and ipsilateral ear discomfort • GP Palpated enlarged Left tonsil but no lymphadenopathy • U/S: Large left neck mass • Referral to local ENT surgeon CT head and neck How was Susan treated? Radiation: Chemotherapy: Cisplatin interferes with cell division by mitosis damaged DNA elicits DNA repair mechanisms activation of apoptosis when repair proves impossible Downhill during treatment Chemotherapy side effects: • Severe nausea and vomiting with blood-tinted emesis • ER visit for dehydration, followed by CCAC and home care over the weekend for IV hydration • Declined IV hydration for 1 day lightheadedness, vagal episode, postural drop Restart IV hydration Radiation Side Effects: • • • • • • • Skin irritation Oral mucositis Oral thrush Xerostomia Taste changes Esophagitis Anorexia • • • • • Hoarseness, laryngitis Tooth decay Earache, tinnitus Trismus Fatigue Psychosocial: About cancer diagnosis, ongoing treatment, and responsibilities About not being able to go through with the treatment and not being disease free About not being available for her family members How did we help Susan? G-tube: Medications: • Mucositis Mouthwash • Morphine liquid • Fluconazole • Flamazine 1% Other: • Skin Care Even after treatment ended… Ongoing side-effects • • • • Thick oral secretions Neck edema Decreased hearing Oral thrush Psychosocial • Difficulty transitioning back to work • Depression • Ongoing guilt Ongoing monitoring Palliative Care and End-of-life • Multidisciplinary approach • Provide patients with relief from their symptoms, pain, physical and mental stress Discussion • How can we make cancer care coordination better? • Thoughts about Susan’s care? How could her journey have been better? • What can we change? • How do you envision cancer care in 2025? Acknowledgments Maitry Patel, Dr. Giuliani [email protected]