Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
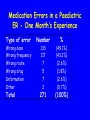
Adverse Drug Reactions in Dentistry (ADRs): Burden of Disease and Special Considerations Michael J. Rieder Section of Paediatric Clinical Pharmacology Children’s Hospital of Western Ontario Division of Clinical Pharmacology Faculty of Medicine & Dentistry University of Western Ontario London, Ontario [email protected] Maria • 6 year old child who had a dental abscess treated in the clinic • Penicillin started 1 week ago • Over the past two days, she has developed fever, malaise and a rash QuickTime™ and a Photo - JPEG decompressor are needed to see this picture. Objectives • Appreciate rate of ADRs • Understand patterns of ADRs to drugs common to dental practice • Appreciate an approach to an ADR associated with dental therapy Perspective on Therapy • God and His Majesty forbid, the fire of the enemy is not half so dangerous as a single drug – M. Platov, 1812 Selective Therapy • Era of selective therapy began in two labs in Europe – Cambridge in 1928 - Sir Alexander Fleming discovery of penicillin – Germany in 1935 - Gerhard Domagk - discovery of sulfanilamide • Demonstration of antimicrobial activity • Serenpedity at work - neither investigator was trying to find an antibiotic Changes in the Paradigm • Demonstration of antimicrobial activity of major importance • Illustration - therapy of Strep. meningitis consisted of rabbit serum, supportive therapy and prayer • Infectious deaths common • Medical paradigm - care, not cure Changes in Care - Consequences • Sulfanilamide activity described in 1935 • Widespread clinical use by 1937 • Major change in clinical care paradigms – In first 10 years of use, 10,000 lives saved in UK among children who would have died of Strep. Infections – Care becomes Cure (Lewis Thomas, Reflections of a Biology Watcher) Elixir of Sulfanilamide Tragedy • Sulfanilamide dissolved in ethylene glycol to improve palatability • Ethylene glycol - a potent nephrotoxin • No pre-marketiug toxicity studies done • Approximately 170 deaths from renal failure, mostly among children • Responsible chemist committed suicide • Major issue in Congress - led to changes that led to current drug regulatory system Introduction • Adverse Drug Reactions are a common and important clinical problem • Seen in 5% of patients treated • Responsible for 5% of all hospital admissions – JAMA 1998; 279: 1200-5 98,000 people in the USA die each year as a result of medical errors ADRs in Dentistry • Relatively little data with respect to ADRs in Dental practice compared to Medical practice • What data is present suggests that overall rates may be similar • No a priori reason to assume different rates ADR Rates • Overall, rate of ADRs in dental patients appears to be similar to adults • Risk appears to relate to known risk factors – Int J Clin Pharmacol Ther 1988; 36: 530-3 Risk Factors for ADRs • History of a previous ADR • Polypharmacy • Impairment of the organs of excretion (hepatic or renal dysfunction) • Extremes of age • Female gender History of ADRs • Elixir of Sulfanilamide Tragedy, 1937 • Chloramphenicol Grey Baby Syndrome, 1950’s • Thallidomide Teratogenicity, 1960’s • Drug substitution errors 1980’s • Ten-fold errors 1990’s • Molecular Misadventures ADR Classification • ADRs often called “drug allergy” • Immune involvement is common, but true drug allergy is relatively rare • Mislabelling leads to therapeutic confusion Hypersensitivity Gell & Coombs Type I Mast Cell IgE Vasodilation Smooth Muscle Contraction Chemotaxis Degranulation Urticaria Bronchoconstriction Hypotension - Shock Inflammation Hypersensitivity Gell & Coombs Type II NK Cell IgG Cell lysis Phagocytosis Phagocyte Complement Removed by Reticuloendothelial System Hypersensitivity - Gell & Blood Coombs Type III Vessel IgG Complement Immune Complexes Phagocyte Reactive Oxygen Species Inflammation Type IV Hypersensitivity Sensitisation Antigen Presenting Cell Immunologic Memory Target Cell Cytotoxic T Cell Cytokines Inflammation Macrophage Cell Destruction Gell and Coombs • Elegant, erudite classification system • Mechanistic • Sadly, does not address the vast majority of ADRs ADR Classifications • A number of schemes have been proposed • Unfortunate and common use of the term allergy • Patterson, DeSwarte and Greenberger (1986) – Predictable – Unpredictable • New England Review of Allergy Proceedings, 1986, 7: 325-42 Predictable ADRs • Predicated on and predictable from the drug’s pharmacology – – – – Side Effects Secondary Effects Interactions Toxicity Unpredictable ADRs • Not known to be related to the drug’s pharmacology – – – – Intolerance Allergic - Pseudoallergic Idiosyncratic Psychogenic Predictable ADRs • Side Effects – Fine tremor associated with inhaled salbutamol (albuterol) • Secondary Effects – Pseudomembranous colitis after lincomycin therapy • Interactions – Bleeding when coumadin and cimetadine are given concurrently • Toxicity – Metabolic acidosis in salicylate overdose Unpredictable ADRs • Intolerance – Intractable vomiting associated with erythromycin therapy • Allergic - Pseudoallergic – Anaphylaxis or urticaria associated with pencillin therapy • Idiosyncratic – Stevens-Johnson Syndrome associated with sulphonamides • Psychogenic – Environmental Hypersensitivity Commonly Used Drugs • • • • • Penicillins Opiates Local Anaesthetics Acetaminophen NSAIDs Penicillins • Can cause all four types of Gell & Coombs reactions • Commonest is Type I (hypersensitivity) • Said to occur in as many as 10% of patients Penicillins • Most common ADRs are skin rash and diarrhoea • Diarrhoea usually self resolving • Rash may be allergic or may be drugdisease interaction Penicillins • Stated incidence of allergy 10% • Actual incidence probably much lower • ADRs described probably represent viral-drug interactions • Can be verified or refuted with skin testing Penicillins • Penicillin skin testing available at selected centres • Testing requires use of both minor and major determinants • Accurate in even small infants • Often deferred until several years after an event Percentage Time Opiates • Commonly used for severe pain • Dose-related respiratory depression in high doses • About 5% of the population develops urticaria on usual doses • NOT an allergy - reflects sensitivity • Crosses the class Local Anaesthetics • Commonly and widely used • Two common problems - inadvertent intravenous injection and allergy • Allergy tends to be unique to class (amide or ester) • Can be tested for Skin Testing • Commonly used • Role is to determine safety, not causation • Hence, usually uses agents of the other class Local Anaesthetic Sensitivity • Ocassionally involves both classes • A considerable problem for the practicing dentist • Benadryl may be used instead modestly effective Acetaminophen • • • • Commonly used Very safe in usual therapeutic doses Only dangerous in overdoses Can occur in setting of repeated suproatherapeutic dosing NSAIDs • Commonly used and increasingly used among children and adolescents • Associated with GI bleeds, gaastrointestinal discomfort • Can be associated with hypersensitivity NSAIDs • Can be cross-class • In this case, may need to use therapeutic alternatives Other Agents • Macrolides - can be associated with vomiting and GI upset • Most common with erythromycin, less common (but not unknown) with newer agents • Clindamycin - diarrhoea more common than with other agents Special Cases • Drug Substitution • 10 fold errors – Unique problem in Paediatrics – More common among certain staff • Drug Errors – Probably more common in children than adults – Again, may be more common among certain staff Medication Errors in a Paediatric ER - One Month’s Experience Type of error Number % Wrong dose Wrong frequency Wrong route Wrong drug Information Other 133 117 7 5 7 2 (49.1%) (43.2%) (2.6%) (1.8%) (2.6%) (0.7%) Total 271 (100%) Medication Errors • Paediatric doses need to be individualized • Knowledge of paediatric doses often much less than optimal • Certain staff - trainees, those unused to working with children, mathematically inept - at higher risk Unique Cases • Special cases arise in which ADR patterns are not the same in children as in adults Cefaclor-associated serum sickness - seen in 1% of children treated, but probably 0.1 to 0.01% of adults -Can J Clin Pharmacol 1999; 6: 197-201 Pre-Marketing Research • Pre-clinical use often includes juvenile animals • Classically, Phase I - III trials include 300 to 5000 patients • Hence, will NOT detect rare but potentially serious events (e.g. most drug-induced hypersensitivities) Limitations of Usual Data • Use of usual data sources for ADR assessment (e.g. CPS) significant • However, usual data sources (e.g. CPS) are poor sources of ADR information – Common events not reported – Rare events over-stated Implications • Novel or serious ADR patterns to new drugs may not be appreciated based on the pre-marketing data available • The CPS may not help you much • Vigilance is important, especially for novel agents Approach to an Undesired Event • Careful Clinical Approach • Evaluation of therapeutic goals – Have we achieved the goal? – If not, how are we going to achieve the goal? – Do we need to revise our goals or do we need to revise our strategy? Clinical Approach to a Possible ADR (I) • History and Physical Examination – Drug, dose, timing, rationale, other events • • • • Analysis of Drug Exposure Differential Diagnosis Obtaining Information Coming to a Clinical Opinion Clinical Approach to a Possible ADR (II) • • • • • Confirmation Communication Treatment Reporting Coping – Patient – Patient-physician relationship References • Patterson R, DeSwartre RD, Greenberger PA et al.: Drug allergy and protocols for management of drug allergies. New England Review of Allergy Proceedings 1896; 7: 325-42 • Rieder MJ: In vitro and in vivo testing for adverse drug reactions. Pediatric Clinics of North America 1997; 44: 93-111 • Gupta A, Waldhauser L: Adverse drug reactions from birth to early childhood. Pediatric Clinics of North America 1997; 44: 79-92 What About Maria? • Stevens-Johnson Syndrome • Pathogenesis related to bioactivation of drug to a reactive intermediate and then (probably) immune propagation • Issues - multi-organ involvement, risk of infection • Therapy - supportive, monitoring for complications, possible use of pulse corticosteroids QuickTime™ and a Photo - JPEG decompressor are needed to see this picture. Take Home Message • • • • Know the drugs that you are using Be vigilant When in doubt, ask When faced with a dilemma, seek expert opinion Acknowledgments • Canadian Institutes of Health Research MRC • Kidney Foundation of Canada • Hospital for Sick Children Foundation • Drs. Gideon Koren, Doreen Matsui, Shinya Ito, Greg Kearns, Bruce Carleton, • Drs. Sanford Cohen, Neil Shear, Ralph Kauffman, Stuart MacLeod