Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
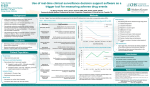
02/15 Development and Validation of a Prognostic Model for predicting Adverse Drug Reactions in Children HERGIBO F., MIMOUNI Y., LAJOINIE A., CASTELLAN A-C., KASSAI B., NGUYEN K.A. INSERM CIC 201, EPICIME, Laboratoire de Biométrie et Biologie Evolutive UMR5558 CNRS-Université Claude Bernard Lyon 1, Hospices Civils De Lyon, Lyon, France Introduction Adverse Drug Reactions (ADRs) detected by spontaneous report are underreported Others methods Chart review Cooperation between the pharmacovigilance team and clinicians Direct observation “Trigger tools”: data element within health records that may identify or predict an AE (clinical, medication or laboratory data) associated with chart review Prognostic model: strategy to predict and prevent ADRs 2 studies in adults (Bates 1999, Evans 2005) None in children Bates et al. 1999 Methods Nested case-control study within a cohort 4108 admissions 11 units (stratification, randomization) 2 hospitals 6 months 2 levels of analyses: limited set of variables available for all patients using computerized data from 1 hospital larger set of variables for the case patients (with an ADE) and matched controls (same unit with the most similar pre-event length of stay) from both hospitals Outcomes: presence of an ADE, preventable ADE or severe ADE Results Independent Predictor Cohort Analysis All ADEs Preventable ADEs Case-control Analysis OR (CI95%) Electrolyte concentrate 1.7 (1.1 - 2.5) Diuretic 1.7 (1.0 - 2.6) Medical ward admittance 1.6 (1.1 - 2.3) Platelet category 4.5 (1.6 - 12.9) Antidepressant 3.3 (1.3 - 7.9) Antihypertensive agent 2.9 (1.4 - 4.4) Medical ward admittance 2.2 (1.1 - 4.4) Electrolyte concentrate 2.1 (1.1 - 4.1) Independent Predictor OR (CI95%) All ADEs Exposure to psychoactive drugs 2.1 (1.3 - 3.6) Severe ADEs Cardiovascular drugs 2.4 (1.3 – 4.5) Small number of patients Little power of predictors No generalizability to other care settings: variation of data from site to site No specific patient groups and type of events Risk stratification approach unlikely productive Limitations Evans et al. 2005 Methods Conditional logistic regression Analysis of ADEs by therapeutic class of drugs and severity 10 year 1 hospital Case matched with up to 16 control patients Results Risk Factor Patients Characteristics 4376 ADEs Drug Administration Patient Type OR (CI95%) Female 1.5 – 1.7 Age 0.7 – 0.9 Weight 1.2 – 1.4 Creatinine Clearance 0.8 – 4.7 Number of Comorbidities 1.1 – 12.6 Dosage 1.2 – 3.7 Administration Route 1.4 – 149.9 Number of Concomitant drugs 1.2 – 2.4 Service 1.2 – 4.9 Nursing Division 1.5 - 3.8 Diagnosis-related Group 1.5 – 5.7 The computer-prompted method of surveillance of ADEs may have systematically missed certain categories of ADEs Limitations Antineoplastic agents and anesthesia probably underreported No access to nurse staffing levels: no increased patient census, patient turnover, and nursing acuity as risk factors Liver disease was not identified as a significant risk factor for ADEs; this may be due to misclassification Objectives Primary objective: To develop and validate the EREMI trigger tool prognostic model for predicting of ADRs in a hospitalised paediatric population Secondary objective: To describe the ADRs detected by the model (by age groups, medications the most incriminated, the most frequent ADRs) Method Study Design Database study (EREMI data) EREMI: observational, multicenter, prospective study which assesses the relationship between ADRs and unlicensed/off-label drug use in hospitalized children Study Population EREMI Patients Inclusion Criteria Children 0-15 years EREMI patients enrolled from September 2013 to December 2014 in Lyon > 3 days hospitalisation > 1 drug administration Wards: Nephrology Exclusion Criteria Patients hospitalized for an ADR Patients undergoing voluntary drug detoxification Psychopathology + patients > 15 years or hospitalized < 3 days Endocrinology Patients aged 15 or more Pneumology high accidents, suicide Neurology Hepato-gastrology Rheumatology Pediatric reanimation death rate: violence, Patients who did not take any drugs during their hospital stay Ethics - EREMI Funded by the ANSM Favourable opinion of the CCTIRS on 03/10/2013 Subjected to an authorization application from the CNIL Consent not required: information sheet sufficient to meet regulatory requirements CPP submission is on going Electronic chart review process for ADR detection and validation Medical records Prescriptions ● Medical history ● Prescribed drugs ● Cause of hospital admission ● Administered drugs ● Clinical observations ● Hospital discharge report Active Centralized ● Dosing regimen ● Drug-Drug Interactions Detection Health exam & lab test results ● Physiological functions ● Biological examinations ● Evolution of the results Trigger Tool Original Trigger Tool Data Flow Licensed/UL/OL Classification Theriaque EREMI Hospital Database Centralised Age Coded Hospital stay Database Administered drugs Height Weight Lab results ADR: Active detection Diagnoses etc. Nominal data ADR: spontaneous reports ADR Detection & validation Pharmacovigilance Regional Centers Pharmacovigilance Independent Board Cross validation Summary of Triggers Variable Trigger Age Weight Demographic variables Height BMI Underweight, Overweight Creatinine plasma levels Hypercreatininemia, Renal failure, toxicity Administered drugs Overdosage (antidotes), hypoglycemia Routes of administration or hyperglycemia (inulin), hemorrhage Doses or Diagnoses (antiemetics), blood clot (heparin), vomiting allergic reaction (antihistaminics), withdrawal syndrome Variable Trigger Variable Trigger Temperature Hypothermia, Hyperthermia, Fever Calcium Hypocalcemia, Hypercalcemia Blood Pressure Hypotension, Hypertension Drug Dosage Toxicity Oxygen Saturation Hypoxia Chlorate Anemia Phosphate Leucopenia, hyperleucocytosis Anionic gap Metabolic acidosis Neutropenia, neutrophilic Serum Glucose Hypoglycemia, Hyperglycemia hyperleucocytosis Urea Renal failure/toxicity Eosinophils Hypereosinophilia Uric acid Platelets Thrombocytopenia ASAT Total IgE Allergic reaction ALAT Liver failure/toxicity Phosphatase alcaline Hyperbilirubinemia Gamma glutamyl transferase Increased transaminases Hemoglobin Hematocrit Leucocytes Neutrophils Partial Thromboplastin Time INR Hemorrhage Anti-Xa Magnesium Hypomagnesemia, Hypermagnesemia Hypochloremia, Hyperchloremia Hypophosphoremia, Hyperphosphoremia Total bilirubin D-dimer Blood clot Triglycerides Sodium Hyponatremia, Hypernatremia LDH Potassium Hypokalemia, Hyperkalemia Lipase Hyperlipidemia Selection of Variables Training Set Multivariate Analysis p < 0.10 Intermediate Model 2/3 patients Univariate Analysis p < 0.20 Final Model Discrimination Calibration Validation Set 1/3 patients Conclusion Define pronostic value of physiological and biological triggers in hospitalized children Further step: external validation with EREMI patients from Paris Contribute to the development of an automated trigger tool Thank you TRAINING SET 2/3 of the patients Selection of variables/triggers - Demographic - Medication Prognostic Model Statistical Analysis - Laboratory Method for accounting missing values Univariable analysis p<0.20 VALIDATION SET 1/3 of the patients Discrimination - Sensitivity, Specificity, predictive value Multivariable analysis p<0.10 - C-statistic (ROC) Backward stepwise regression Calibration Final multivariate model of triggers Risk score