Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Compounding wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Toxicodynamics wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Drug design wikipedia , lookup
Theralizumab wikipedia , lookup
Ciclosporin wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacovigilance wikipedia , lookup
Pharmacogenomics wikipedia , lookup
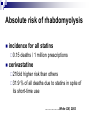
Drug interactions Jiří Slíva, M.D., PhD. Agenda epidemiology classification and mechanism of drug interactions (DI) recent cases cisapride, statins, grape-fruit juice, St. John´s worth etc. quality of information on DI Epidemiology of DI hospitalized 7 % of ADRs during hospitalization 0.2 % serious and life-threatening DI ambulatory follow-up of 2422 patients during 2 months 4.7 % potentially risky combinations 0.3 % DI Definition & classification LI =…administration of substance (drug) A influences substance B pharmacodynamic DI – change of effect without influence of pharmacokinetics pharmacokinetic DI – influence of pharmacokinetics clinically important / unimportant advantageous (analgesics, antihypertenzives, ICS + LABA) harmful synergic / antagonistic Pharmacodynamic interactions Diuretics + digoxine: hypokalemia - toxicity of glycosides IMAO + ephedrine, thyramine: hypertensive reaction warfarine + ASA (NSAIDs): bleeding NSAIDs + antihypertensives: antihypertensive effect non-sedative antihistaminics + alcohole: sedace Parmacokinetic interactions Absorption Distribution Biotransformation Excretion Absorption Influence of GI motility, stomach evaluation acceleration - metoclopramide, cisapride deceleration - atropine, opioids Inhibition of resorption cholestyramine x warfarine, digoxin epinephrine in local anesthetics Distribution Plasma protein binding – mostly clinically non-important (+ elimination) ASA, NSAIDs, OADs, sulfonamides, fenytoine phenylbutazone x warfarine = displacement from a bound to albumine + inhibition of metabolism of Swarfarine salicylates secretion + methotrexat: + inhibition of tubular Biotransformation Cytochrome P-450 - isoenzymes CYP 3A4, 2D6, 1A2, 2C9 INDUCTION (barbiturates, rifampicine, fenytoine, carbamazepine, ethanole) INHIBITION (cimetidine, macrolides, imidazoles, SSRIs, grape-fruit juice – 3A4; 2D6 - verapamile, amiodarone) Xantinoxidase - allopurinole x azathioprine Aldehyddehydrogenase - disulfirame x warfarine Different contributions of various CYP isoforms in liver in total active in drug metabolism Genetic polymorphism metabolisers – slow, intermediary, fast, ultra-fast CYP 1A2, 2C9, 2D6, 2E1 xantinoxidase, alcoholdehydrogenase, COMT, AChE phenotypisation – individualized therapy Excretion Change of plasma protein binding - free fraction - filtration - excretion Inhibition of tubular secretion probenecide x peniciline, AZT Change of volume & pH of urine diuretics Genetic susceptibility to ADRs pharmacogenetics Mibefradil CCB blocking Tchannels – hypertension, CHF 1997 recall after 1 year due to DI historically first recall due to DI only, minimal toxicity strong inhibitor of CYP3A4 DI and risk of QT interval prolongation cisapride non-sedative antihistaminics – astemizole, terfenadine …..ventricle arrhythmias – torsade de pointes ………..fibrilation !!! astemizole, terfenadine…….recall cisapride …..recall DI of statins & rhabdomyolysis cerivastatin recall due to rhabdomyolysis and interactions with CYP3A4 inhibitors and fibrates (gemfibrozile) imidazoles, macrolides, diltiazem, verapamil, ciclosporin, grapefruit etc. Rhabdomyolysis due to DI of statins and fibrates August 2001 – recall of cerivastatine as a result of high risk of rhabdomyolysis most lipophilic and highest bioavailability (60 %) in USA very often combined with gemfibrozile administered at relatively high doses Absolute risk of rhabdomyolysis incidence for all statins 0.15 deaths / 1 million prescriptions cerivastatine 21fold higher risk than others 31.9 % of all deaths due to statins in spite of its short-time use ……………….White CM, 2002 Food supplements, phytopharmacs Grape-fruit juice an St. John´s wort an inhibitor of 3A4 inductor of 3A4 smoking – induction of 1A2 (imipramine, clozapine, propranolole) ethanole - 2E1 Interesting DI I. Crataegus levigata, Cr. monogyna (hawthorn) concomitant administration with digoxine at dose 0.25 mg for 10 days or combination of digoxine with an extract of leaves & flowers 450 mg bid (1 dose = 84.3 mg of oligomeric procyanides) led to decrease of maximal plasma concentration of digoxine by 14 % and minimal plasma concentration by 23 % Mechanism of DI – influence of P-glycoprotein …Tankanov R, 2003 Interesting DI II. Ginseng higher risk of bleeding when combined with warfarin …Janetzky K, 1997 lower efficacy of diuretics …Becker BN, 1996 higher pl. levels of digoxine …Mc Rae S, 1996 Interesting DI III. Gingko biloba 2 case reports of fatal bleeding: man, 71 y, ibuprofen 600 mg/d, Gingko biloba 40 mg bid, 4 weeks => fatal intracerebral bleeding woman, 70 y, warfarin for 5 y, then 2 months Gingko biloba => intracerebral bleeding …Matthews MK, 1998 Mechanism of DI – inhibition of PAF etc. stimulation of CYP2C19 – faster metabolism of omeprazole …Yin OQ, 2004 Interesting DI IV. Hypericum perforatum Mechanism of DI pharmacokinetic - induction of cytochrome P450 in liver (esp. CYP1A2, CYP2C9 & CYP3A4) - induction of P-glycoprotein - inhibition of MAO pharmacodynamic - in synapsis – elevation of 5-HT – DI with triptans, antidepressants Interesting DI V. Hypericum perforatum Drugs Result of DI antihistamines (fexofenadin, loratadine) lower efficacy (fexofenadine), delirium (loratadine) antivirotics (efavirenz, indinavir, lamivudin, nevirapin, stavudin) lower virostat eff. digoxine lower eff. of digoxine imatinibe lower eff. of imatinibe immunosuppressants (ciclosporin, tacrolimus) lower immunosuppressive eff. midazolam lower eff. of midazolam peroral contraceptives gravidity, womb bleeding simvastatine lower lipid-lowering eff. SSRI, triptans, dextromethorphane serotonin syndrome verapamile lower eff. of verapamile warfarine lower anticoagulatory eff. Grape-fruit juice a strong inhibitor of CYP3A4 & Pglycoprotein Where do I find information about DI ? Selected resources: BNF & AISLP – SPCs database Micromedex – accessible via Onelog Stockley’s Drug Interactions Interakce InfoPharm Quality of information about DI Clinical relevance: A...probably non-serious B…so far not confirmed (theoretical) C…moderate D…serious Level of documentation 1...uncomplete case-reports 2…good documented case-reports reports 3…studies with healthy volunteers 4…controlled study with patients or series of case- Adverse drug reactions (ADRs) Reasons of ADRs Drug Patient Inappropriate drug combination Inappropriate indication Classification of ADRs I. Serious Death /life threatening Nonserious Serious deterioration of health Permanent aftereffect Hospitalization Hospitalization prolongation Disability Congenital abnormality Others Classification of ADRs II. Expected Unexpected ADRs mentioned in current SmPC Others PSUR (Periodic Safety Update Report) Legislative in EU (Eudralex Vol. 9 Pharmacovigilance, Commission Directive 2001/20/E, CPMP/PhVWP/108/99 etc.) + local requirements of regulatory authorities Pharmacovigilance registration holder regulatory body health professionals System of reporting in the Czech Republic Registration holder Health professionels Serious ADR Serious or unexpected ADR Serious ADR (up to 15 d.) Non-serious ADR (PSUR) Reg. author. Minimal data needed for ADR reporting Drug suspected Patient information (age, sex) Reaction description Source of reporting