Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
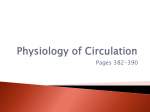
Education Module Learner Assessment July 06 Page CME Credit Expired 1 2 3 4 5 6 7 8 9 10 My Learning Plan Neo Editorial Plus Overview Board 2006 1 Your Score Back to NeoReviews Mainpage January 06 2 February 06 3 March 06 4 April 06 5 May 06 6 June 06 7 July 06 8 August 06 9 September 06 10 October 06 November 06 December 12 06 11 A 38-year-old primiparous woman is in her 24th week of pregnancy. Fetal ultrasonography reveals generalized skin edema, bilateral pleural effusions, and mild ascites. Mother's blood type is O Rh-positive. You discuss with medical students the pathophysiology of interstitial fluid accumulation characteristic of hydrops in this fetus. Of the following, the factor MOST protective against interstitial fluid accumulation is high: capillary filtration coefficient capillary hydrostatic pressure central venous pressure interstitial oncotic pressure osmotic reflection coefficient You selected , the correct answer is . Do you want to add anything to your Learning Plan? (You must be an AAP member or PediaLink ® Learning Center Subscriber to use this feature.) Hydrops fetalis is defined as excessive accumulation of interstitial fluid in the fetus. With the successful implementation of strategies for prevention and treatment of Rh blood group isoimmunization, approximately 90% of the cases of hydrops fetalis currently are of the nonimmune type, as in the fetus in this vignette. A review of the regulation of fluid movement between vascular and interstitial spaces may facilitate our understanding of the pathophysiology of hydrops fetalis. Interstitial fluid balance (Figure 1) Figure 1 http://emb.aap.org/courseprodv2/Index.asp[4/4/2012 4:05:35 PM] Education Module Learner is determined by the rate of formation of the interstitial fluid from the vascular compartment and the rate of its drainage through the lymphatic system. Let us examine first the interstitial fluid formation and then we will return to review the interstitial fluid drainage. The driving forces for fluid extravasation from the vascular space to the interstitial space are the hydrostatic pressure within the capillary (P C) and the colloid oncotic pressure within the interstitial fluid (p i). Conversely, the driving forces for fluid return from the interstitial space to the vascular space are the hydrostatic pressure within the interstitial fluid (Pi) and the colloid oncotic pressure within the capillary (p C). Thus, the higher the hydrostatic pressure gradient (?P = P C P i), the greater is the rate of interstitial fluid formation. Conversely, the lower the colloid oncotic pressure gradient (?p = p C - p i), the greater is the rate of interstitial fluid formation. Two characteristics of the capillary influence the fluid flux: capillary filtration coefficient (CFC) and osmotic reflection coefficient (s). The former, CFC, is a product of capillary surface area and capillary hydraulic conductivity; whereas the latter, s, is a measure of capillary endothelial permeability. The higher the capillary surface area and the capillary hydraulic conductivity (ie, the higher the capillary filtration coefficient), the greater is the rate of interstitial fluid formation. On the other hand, the higher the osmotic reflection coefficient (s) (ie, lesser capillary endothelial permeability), the lower is the rate of interstitial fluid formation. The colloid oncotic pressure in the vascular and interstitial spaces depends on the concentration of osmotically active particles in each compartment and the permeability of the intervening capillary endothelium. The less permeable the endothelium, meaning high s, the greater is the separation of osmotic particles and the greater is the efficacy of colloid oncotic pressure difference in preventing fluid flux toward the interstitial space. Conversely, the more permeable the endothelium, meaning low s, the greater is the equilibration of osmotic particles and the lesser is the efficacy of colloid oncotic pressure difference in preventing fluid flux toward the interstitial space. The fluid movement between the vascular space and the interstitial space is summarized by the following equation: Jv = CFC (?P - s?p) http://emb.aap.org/courseprodv2/Index.asp[4/4/2012 4:05:35 PM] Education Module Learner in which Jv is the fluid flux across the capillary, CFC is the capillary filtration coefficient, ?P is the hydrostatic pressure gradient (P C - P i), s is the osmotic reflection coefficient, and ?p is the colloid oncotic pressure gradient (p C - p i). The fetus, in contrast to the adult, is much more susceptible to interstitial fluid accumulation for the following reasons: First, the capillary filtration coefficient is about fivefold higher in the fetus than in the adult. Second, the interstitium of the fetus is much more compliant than that of the adult, that is, the interstitial space is capable of accumulating a large amount of fluid with only a small increase in the interstitial hydrostatic pressure. This low P i accounts for a higher ?P in the fetus. Third, the fetal capillary is more permeable to plasma proteins. The effect of this enhanced solute permeability is that for any given solute concentration difference across the capillary endothelium, the colloid oncotic pressure difference drives fluid less effectively from the interstitium to the vascular space. Fourth, the plasma protein concentration is lower in the fetus than in the adult, which results in a reduced plasma colloid oncotic pressure. Pathologically, any condition that increases the hydrostatic pressure gradient, increases the capillary permeability, or decreases the colloid oncotic pressure gradient is conducive to excessive interstitial fluid accumulation and resultant hydrops. Finally, let us examine the interstitial fluid drainage through the lymphatic system, the second component of the interstitial fluid balance. The lymph flow depends on the anatomic development of the lymphatic system and the pressure gradient between the interstitial fluid space and the venous compartment. In conditions associated with anomalous development of lymphatics (eg, lymphangiectasia) or lymphatic obstruction (eg, thoracic duct occlusion), the interstitial fluid drainage is impaired. Also, a high central venous pressure relative to interstitial hydrostatic pressure impairs lymph flow. In the fetus, lymph flow ceases when the central venous pressure exceeds 10 mm Hg in contrast to approximately 25 mm Hg in the adult. Pathologically, any condition that alters the lymphatic system, or that increases the central venous pressure is conducive to impaired interstitial fluid drainage and resultant hydrops. In this vignette, among all the factors that determine the interstitial fluid balance, the factor most protective against interstitial fluid accumulation and resultant hydrops is high osmotic reflection coefficient. Do you want to add anything to your Learning Plan? (You must be an AAP member or PediaLink ® Learning Center Subscriber to use this feature.) References: Apkon M. Pathophysiology of hydrops fetalis. Sem Perinatol. 1995;19:437-446 Bukowski R, Saade GR. Hydrops fetalis. Clin Perinatol. 2000;27:1007-1031 Carlton DP. Pathophysiology of edema. In: Polin RA, Fox WW, Abman SH, eds. Fetal and Neonatal Physiology. 3rd ed. Philadelphia, Pa: WB Saunders; 2004:13571361 American Board of Pediatrics Content Specification(s): http://emb.aap.org/courseprodv2/Index.asp[4/4/2012 4:05:35 PM] Education Module Learner Know the differential diagnosis and the plan of management of a fetus with nonimmune hydrops http://emb.aap.org/courseprodv2/Index.asp[4/4/2012 4:05:35 PM]