Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
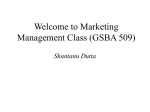
Office Use AVERAGE BP SCORE Add Systolics divide by number of readings Add Diastolic divide by number of readings Home Blood Pressure Monitoring Name: Date of Birth: Telephone number: Address: Date Day 1 Time Systolic BP (Upper Number) Diastolic BP (Lower Number) Pulse Rate am pm Day 2 am pm Day 3 am pm Day 4 am pm Day 5 am pm Day 6 am pm Day 7 am pm Please use this sheet along with your BP machine to record your blood pressure at home. Ensure you are relaxed when checking your BP. It is generally better to have been quietly sitting for 5 minutes before checking your BP. Please check your blood pressure morning and night for seven days and then return the record sheet to the Surgery. If you are already taking medication please take morning readings after your tablets and evening readings after medication.