Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
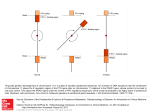
Letters to the Editor * Address correspondence to this author at: St. Savas Oncology Hospital Nuclear Medicine Department 171 Alexandras Ave. Athens 115 22, Greece e-mail [email protected] DOI: 10.1373/clinchem.2007.102194 Acute Variation of Osteocalcin and Parathyroid Hormone in Athletes after Running a HalfMarathon To the Editor: Fig. 1. Box and whisker plots of the derived PTH 95% CIs for patients on L-thyroxine therapy. (A), Patients (n ⫽ 64) with excessively suppressed TSH (⬍0.4 mIU/L) concentrations [mean (SD) TSH ⫽ 0.29 (0.14) mIU/L]. The true calcium concentration (albumin-corrected) for this group of patients was 9.61 (0.26) mg/dL. (B), Patients (n ⫽ 31) with TSH concentrations within reference limits [mean (SD) TSH ⫽ 0.87 (0.36) mIU/L). Means of the PTH concentrations for each group were compared with the application of the t-test for independent samples, with logarithmic transformation of data, assuming unequal variances (Welch-test, P ⫽ 0.0197). Data for the healthy blood donors (n ⫽ 39) are not shown. needed to confirm our observation and to clarify its underlying mechanism. Knowledge of this effect may help clinicians to avoid unnecessary and expensive work-ups for suspected hyperparathyroidism. Grant/Funding Support: None declared. Financial Disclosures: None declared. References 1. Aloia JF, Feuerman M, Yeh JK. Reference range for serum parathyroid hormone. Endocr Pract 2006;12:137– 44. 2. Pantazi H, Papapetrou PD. Changes in parameters of bone and mineral metabolism during therapy for hyperthyroidism. J Clin Endocrinol Metab 2000;85:1099 –106. 3. Kumeda Y, Inaba M, Tahara H, Kurioka Y, Ishikawa T, Morii H, Nishizawa Y. Persistent increase in bone turnover in Graves’ patients with subclinical hyperthyroidism. J Clin Endocrinol Metab 2000;85:4157– 61. 4. Corbetta S, Lania A, Filopanti M, Vicentini L, Ballaré E, Spada A. Mitogen-activated protein kinase cascade in human normal and tumoral parathyroid cells. J Clin Endocrinol Metab 2002; 87:2201–5. 5. D’Amour P, Räkel A, Brossard JH, Rousseau L, Albert C, Cantor T. Acute regulation of circulating parathyroid hormone (PTH) molecular forms by calcium: utility of PTH fragments/PTH(1– 84) ratios derived from three generations of PTH assays. J Clin Endocrinol Metab 2006;91:283–9. Adonios Zanglis* Demetrios Andreopoulos Nikolaos Baziotis St. Savas Oncology Hospital Nuclear Medicine Department Athens, Greece Parathyroid hormone (PTH) and osteocalcin (OC) play important roles in bone remodeling and bone metabolism. Although the physiological functions and clinical significance of these markers are well established, the influence of other biological variables aside from diurnal and seasonal variability has been less well investigated (1 ). Because little information is available on the kinetics of such markers after physical exercise, we measured PTH and OC in 15 athletes performing a half-marathon run. The study population consisted in 15 healthy trained white males, (mean age, 47 years) who had been engaged in specific endurance training for at least 5 years. Participants performed a 21-km, half-marathon run under competition conditions, while equipped with a heart-rate monitor [mean (SE) VO2 max 85% (3%)]. Prior to the race, preexercise baseline fasting blood samples were collected from the volunteers after a 48-h rest from the last training, 30 min before they warmed up for the race. Post exercise samples were collected immediately after the race, and 3 h, 6 h, and 24 h thereafter. All study participants gave informed consent for being tested, and the study was approved by the ethics Clinical Chemistry 54:6 (2008) 1093 Letters to the Editor committee. Blood was collected in vacuum tubes containing no additives (Becton Dickinson) and centrifuged at 1500g for 10 min at room temperature, and the serum was immediately analyzed. OC and intact PTH were measured on an Elecsys 2010 by electrochemiluminescence immunoassays (Roche Diagnostics GmbH). We used the N-MID Osteocalcin assay that is specific for intact OC (amino acids 1– 49) and the main N-terminal fragment (amino acids 1– 43) resulting from proteolytic cleavage after blood collection. Among markers of bone turnover, OC was selected to verify the effects of physical training on osteoblast function, because it may indirectly reflect acute changes in cortisol, and it is currently considered an indirect marker of growth hormone abuse in sports (2 ). The total assay imprecision (CV) was 1.1%–5.9% for OC and 1.7%–5.5% for intact PTH, respectively (3 ). The ageand sex-specific reference ranges were 1.6 – 6.9 pmol/L for PTH and 14 – 42 g/L for OC, respectively. Hematocrit and hemoglobin were measured on an Advia 120 (Bayer Diagnostics). Because the estimated decrease in total body water does not differ from the percentage plasma volume change (%PVC), results were adjusted for the %PVC, calculated from pre- and postexercise levels of hematocrit and hemoglobin (4 ). The Wilcoxon signed-rank test was used to evaluate the significance of exercise-induced variations during the study period. Data with a nongaussian distribution were normalized using a logarithmic transformation before analysis, and the level of statistical significance was set at P ⬍ 0.05. Data are presented as geometric mean (SE). The concentrations of both markers increased significantly by nearly 1.2-fold (OC) and 2.1-fold (PTH) immediately after the run, but 3 h thereafter rapidly returned to values comparable to those measured before the run (Table 1). The number of participants with values above the respective reference ranges remained stable throughout the study period for OC (n ⫽ 2, 13%), whereas it increased from 0 (0%) to 6 (40%) immediately after the run and returned to 0 (0%) 3 h thereafter for PTH. These results support the hypothesis that a 21-km run produces an acute and transitory increase of both PTH and OC, which is completely reversed 3 h thereafter. Although earlier studies have investigated PTH and OC after strenuous aerobic exercise, especially marathon and ultramarathon running (5 ), no information is available on the kinetics of these markers following moderately strenuous aerobic physical exer- Table 1. Variation of osteocalcin and parathyroid hormone before (pre), immediately after (post), and 3, 6 and 24 h after a 21-km, halfmarathon run, in 15 male recreational athletes.a Pre Plasma volume change, % Weight loss, % Osteocalcin, g/L Parathyroid hormone, pmol/L 3h 6h 24 h –8.0 (1.0) b –0.4 (1.0) 1.2 (1.1) 3.8 (1.0)b — 8.8 (0.7) b 1.6 (0.7) –0.1 (0.8) –1.7 (0.7)b 22.0 (2.5) 27.3 (3.0)b 21.6 (2.6) 20.2 (2.9) 22.3 (2.5) 3.1 (0.3) b 3.1 (0.3) 3.1 (0.5) 3.2 (0.3) — Post a 6.4 (0.7) Values are presented as geometric mean (SE). Differences from the premarathon values were evaluated by the Wilcoxon signed-rank test. b P ⬍ 0.01, vs the pre-run sample. 1094 Clinical Chemistry 54:6 (2008) cise, such as a 21-km half-marathon run, a distance that is more typically accessible for a general population of active individuals. Although Mouzopoulos et al. observed that PTH concentrations increase by nearly 1.3-fold immediately after 245 km of marathon running, these investigators also reported a significant decrease in OC concentrations. Such differences may be due to different preanalytical conditions (sample matrix and storage) or intensity and duration of the run. The transient suppression in osteoblast function occurring during an ultramarathon run, which has been attributed to increases in cortisol and PTH concentrations (5 ), might not occur during shorter-distance runs. Perhaps athletes should be advised to run a half or a fraction of a marathon to avoid potential harmful effects of strenuous endurance exercise. Because OC is a marker of growth-hormone abuse in sports (2 ), such variations should be acknowledged when evaluating the athletes for clinical or antidoping purposes, because these measurement results should be interpreted as physiological responses to exercise rather than pathology or consequences of unfair practices. Grant/Funding Support: None declared. Financial Disclosures: None declared. References 1. Scharnhorst V, Valkenburg J, Vosters C, Vader H. Influence of preanalytical factors on the immulite intact parathyroid hormone assay. Clin Chem 2004;50:974 –5. 2. McHugh CM, Park RT, Sönksen PH, Holt RI. Challenges in detecting the abuse of growth hormone in sport. Clin Chem 2005;51:1587–93. 3. Schmidt-Gayk H, Spanuth E, Kötting J, Bartl R, Felsenberg D, Pfeilschifter J, et al. Performance evaluation of automated assays for beta-CrossLaps, N-MID-Osteocalcin and intact parathyroid hormone (BIOROSE Multicenter Study). Clin Chem Lab Med 2004;42:90 –5. 4. Maughan RJ, Whiting PH, Davidson RJ. Estima- Letters to the Editor tion of plasma volume changes during marathon running. Br J Sports Med 1985;19:138 – 41. 5. Mouzopoulos G, Stamatakos M, Tzurbakis M, Tsembeli A, Manti C, Safioleas M, Skandalakis P. Changes of bone turnover markers after marathon running over 245 km. Int J Sports Med 2007;28:576 –9. Giuseppe Lippi1* Federico Schena2 Martina Montagnana1 Gian Luca Salvagno1 Giuseppe Banfi3 Gian Cesare Guidi1 1 Sezione di Chimica Clinica Dipartimento di Scienze Morfologico-Biomediche Università di Verona, Italy 2 Sezione di Scienze Motorie Dipartimento di Scienze Neurologiche e della Visione Università di Verona, Italy 3 Istituto Galeazzi e Università di Milano Italy * Address correspondence to this author at: Sezione di Chimica Clinica Dipartimento di Scienze Morfologico-Biomediche Università degli Studi di Verona Ospedale Policlinico G.B. Rossi Piazzale Scuro, 10 37134, Verona, Italy Fax 0039-045-8201889 e-mail [email protected] DOI: 10.1373/clinchem.2007.102657 Rapid Real-Time PCR Detection of HP del Directly from Diluted Blood Samples To the Editor: Anhaptoglobinemic patients have been reported to experience severe anaphylactic reactions to transfusions due to the production of antihaptoglobin (anti-HP) antibodies (1, 2 ). Anhaptoglobinemia in patients homozygous for HP del, which is a deletion of an approximately 28-kb segment of chro- mosome 16 extending from the promoter region of the HP (haptoglobin) gene to exon 5 of HPR (haptoglobin-related protein), has been adequately characterized only recently (1 ). Use of a simple duplex PCR method has detected the HP del allele in East and Southeast Asian populations at frequencies of 1%–3% but this allele has not been detected in African, West and South Asian, and European populations (1, 3, 4 ). Thus, diagnosing HP del homozygosity prior to blood transfusion or the infusion of blood components into individuals from East and Southeast Asian populations is effective for preventing anaphylactoid shock due to anti-HP antibodies. We have developed a simple method that uses a 5⬘ nuclease real-time PCR assay (TaqMan; Applied Biosystems) to detect the HP del allele without having to isolate genomic DNA. The ethics committee of Kurume University School of Medicine approved this study protocol. To distinguish alleles, we performed real-time PCR assays that detect the 2 regions that encompass the HP del breakpoint and the 5⬘ region of HP exon 1, which is deleted in HP del. The 20-L PCR reaction contained 200 mol/L deoxynucleoside triphosphates, 1 L of template (diluted blood or genomic DNA), 0.5 U of Ex TaqHS with its buffer (Takara), and the following primers and TaqMan probes (see Fig. 1 legend for sequences): Hp5⬘-F and -R primers (450 nmol/L); Hp5⬘–TaqMan probe (125 nmol/L) for detecting the 5⬘ region of HP; Hpdel-F and -R primers (900 nmol/L); and Hpdel– TaqMan probe (250 nmol/L) for detecting HP del. The PCR temperature profile was 95 °C for 30 s, followed by 50 cycles of denaturing at 95 °C for 5 s and annealing and extension at 60 °C for 30 s. All oligonucleotides were synthesized by Biosearch Technologies. We mon- itored amplification progress by monitoring the fluorescence at the end of each cycle with an Mx3000P instrument (Stratagene) with excitation and emission wavelengths of 492 and 516 nm (FAM), and 585 and 610 nm (CAL Fluor Red 610). With genomic DNA (5 ng/L) as a template, we used dual-color scatter plots to distinguish individuals previously determined to have the HP/HP, HP/HP del, and HP del/HP del genotypes. Samples with the HP/HP genotype had little FAM fluorescence and plotted along the x-axis, HP del/HPdel samples had little CAL Fluor Red 610 fluorescence and plotted along the y-axis, and HP/HP del samples were located between the homozygote samples in the plot (Fig. 1). To the TaqMan real-time PCR mixture, we directly added 1 L of samples diluted 100-fold with PCR-grade water (previously frozen samples of buffy coat from 47 Indonesians from Surabaya or a freshly drawn blood sample from 1 Japanese individual from Fukuoka). Blood was collected in EDTA-containing tubes (Indonesian and Japanese samples) and in a heparin-containing tube (the Japanese sample). The results from 2 independent experiments showed no discrepancies. In addition, the results obtained with the present TaqMan real-time PCR method were fully concordant with those obtained with a previously described PCR method for the same individuals (i.e., 46 HP/HP individuals and 2 Indonesians with HP/HP del; Fig. 1) (1 ). We previously had collected blood samples from 105 Indonesian individuals from Surabaya and had not found the HP del allele in 58 of these individuals (3 ); however, in the present study we did find 2 HP del alleles among the remaining 47 individuals in this population sample. Thus, the HP del allele is also present in Southeast Asian populaClinical Chemistry 54:6 (2008) 1095