Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
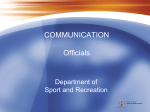
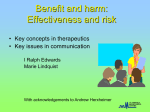
Preventing Patient Harm through Handoffs and Huddles Michelle George, RN MSN CASC 1 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 2 Objectives • Review patient harm events that can occur in the ASC setting • Identify 3 different methods for effective handoff from caregiver to caregiver • Describe the key principles of an effective perioperative team huddle • Identify effective strategies for engaging members of the healthcare team in targeted patient care communications 3 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 4 ASC Industry Clinical Outcomes Trends 1.8 Patient Falls 0.4 0.4 Rate Per 10k Cases Rate Per 10k Cases 1.6 1.4 1.2 1.0 0.8 0.6 0.3 0.3 0.2 0.2 0.4 0.1 0.2 0.1 0.0 0.0 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 '10 '10 '11 '11 '11 '11 '12 '12 '12 '12 '13 '13 '13 '13 '14 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 '10 '10 '11 '11 '11 '11 '12 '12 '12 '12 '13 '13 '13 '13 '14 Patient Wrongs 0.5 0.5 0.4 0.4 0.3 0.3 0.2 0.2 0.1 0.1 0.0 Patient Transfer 14.0 12.0 Rate Per 10k Cases Rate Per 10k Cases Patient Burns 10.0 8.0 6.0 4.0 2.0 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 '10 '10 '11 '11 '11 '11 '12 '12 '12 '12 '13 '13 '13 '13 '14 Note: ASC Quality Collaboration data source 0.0 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 '10 '10 '11 '11 '11 '11 '12 '12 '12 '12 '13 '13 '13 '13 '14 5 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 6 Healthcare Harm: Slips, Trips and Falls Patient harm can occur even when policies & procedures and safety standards have been adopted 7 Healthcare Harm: Surgical Burns Patient harm usually involves commonly used equipment and procedures that are performed on a routine basis Photo Source: http://www.bing.com/images/search?q=medical+errors+surgicalburn 8 Factors in Patient Harm Events • Emotional: Can create feeling of being overwhelmed for the patient, family and the healthcare team • Physical: May involve equipment and/or disposable items that need to be sequestered • Environmental: Team not always alerted by smells, alarms, smoke and other warnings • Political: Egos and opinions can be distracters from the facts during safety breaches • Legal: Company values and policies regarding full disclosure, integrity and commitment to seek resolution serves as the guide through risk management processes 9 Communication Issues Leading Factor in Root Causes Collation of sentinel event-related data reported to The Joint Commission (1995-2005). Available http://www.jointcommission.org/SentinelEvents/Statistics/ 10 Communication Facts • Root cause in majority of patient sentinel events • Miscommunications result in lost information, misinterpretations, and missed actions • Plays role in duplication and omission medication errors • Patient Harm events--direct correlation to communication breakdown during patient hand-offs • Culture issues can lead to failure to speak up • Perioperative setting at high risk due to complex technology complex, involves multiple disciplines, fast paced, and dynamic circumstances 11 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 12 Hand Off Communication Improve patient care by targeting patient handoffs!! 13 Perioperative Continuum of Care Surgeon’s Office OR Scheduling PostOp Visit Discharge Phase Registration PreOp Assessment PACU OR/ Procedure Room 14 Hand Off Communication Tools • Provides structure to communication • Shared model ensures consistency • Ensure that key information is shared • Numerous established tools available • Can be used to improve performance • Requires staff education and practice 15 Hand Off: “5 Ps” • Ensures consistent information is passed during patient transfers • Easy mnemonic to remember • Use the 5 Ps: – Patient – Plan – Purpose – Problems – Precautions 16 Pre-Op OR • Planned surgical Procedure • Antibiotics to be given • Universal Protocol • Significant medical history • Planned anesthesia type • Allergies • Family contact information • Last voided • Equipment needs • Preop medications • Other issues (e.g., NPO, Courtesy of Tripler Army Medical Center. Adapted from OR Manager, April 2006. blood products available) OR • Procedure • Surgeon Plan and Preferences (where we are in the case) • Anesthesia type • Allergies • Significant Medical History • Counts Courtesy of Tripler Army Medical Center. Adapted from OR Manager, April 2006. OR • Irrigation • Medications • Instrumentation on and off field • Specimens on and off field • Equipment needs • Tubes, Lines, Hoses OR Team • Surgical procedure (completed vs. planned) • Anesthesia type • Estimated Blood Loss • Input & Output (e.g., straight catheter, foley) • Allergies • Medications (received intra- PACU • Significant medical history (e.g., contact precautions) • Family contact information? • Equipment needs (e.g., sequential compression devices) • Other issues (e.g., blood op) Courtesy of Tripler Army Medical Center. Adapted from OR Manager, April 2006. products, anesthesia concerns) SBAR Communication Model S Situation Complaint, diagnosis, treatment plan and patient’s wants and needs B Background Vital signs, mental and code status, list of medications and lab results A Assessment Current provider’s assessment of the situation R Recommendation Identify pending lab results and what needs to be done over the next few hours and other recommendations for care 20 Post It Style Communication Tool 21 Engaging the Team SCA’s journey to create a fair and just culture where teammates feel empowered to identify opportunities to improve patient safety and eliminate fear of reporting events that compromise patient safety • The Beginning: – Emerging trend from Root Cause Analysis – Patient safety culture survey results • Purpose: – Prevent healthcare harm from reaching the patient – Shift culture from reactive to proactive – Fully engage team (teammates and practitioners) 22 The Accountability Project Implementation of multi-year program focusing on the prevention of patient harm through enhanced communication and team engagement; rolled out as toolkit Accountability Project I • Focus on culture of safety • Military-style Stand Downs for teammates and physicians • Do No Harm video and training • Speak Up, Speak Out Campaign • Individual and team commitment to prevent patient harm Accountability Project II – Empowering communication training – Retaliation training – Good Catch! Program to reward and recognize team members for identifying and mitigating nearmisses – Repeat patient safety culture survey • Perfect Time Out training • Repeat patient safety culture survey 23 Good Catch! Program • Fun and interesting baseball themed activities • Increased awareness with friendly competition • Sustained engagement by using playoff schedule Center 1 Center 2 Center 3 Center 4 • Tracked and trended “good catches” as PI study focus Center 5 • Individual and team recognition with certificates and plaques Center 7 Center 6 Center 8 Center Winner 1 Center Playoff Center Winner 2 Regional Champion Center Winner 3 Center Playoff Center Winner 4 24 Hand Off Communication Strategies • Determine the best structure for your facility—known tool or unique design • Select the core content to include in hand-offs • Determine who is responsible for initiating hand off communications • Provide training to all team and practitioners • Implement your hand off communication plan • Engage patient and family when appropriate • Leader rounding to determine effectiveness • Assess hand off communications during near-miss and actual event Root Cause Analysis 25 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 26 Key Principles of OR Huddles • Proactive management of problematic situations • Takes time and commitment to resolve problems • Drives accountability • Collaborative decision making process • Provides a voice for every member • Prevents safety issues which decreases cost and improves efficiency, safety and satisfaction • Inspires communication and team work and ultimately the end result is a high standard of patient safety 27 Huddle Types Early Morning Huddles Afternoon Huddles Special Huddles Primary participants are the clinical team members Multidisciplinary participation, usually the same participants every day Special circumstances Review the plan for the day Recap the day’s issues/ address root causes Delays or add-ons in the schedule Address staffing for the day Address schedule changes (diabetics, pediatrics, gaps) Out of order patients Address management of comorbid conditions Review cases for the next day Unanticipated staffing changes Collaborative work between OR team members Ensure equipment, implants, vendors are ready for cases Broken equipment or supply outages Reminder of upcoming events—meetings, inservices, deadlines, etc. Plan for special patient management issues 28 The Ultimate Huddle: Surgical Time Out • All OR team members to participate • Designated leader • Performed immediately prior to the procedure • Stop all other activities • Start over for any interruptions • Address any special conditions or needs • Speak up for information or questions • Do not proceed until all team is in agreement 29 Strategies for Effective Huddles • Determine the best meeting time for the team • Assign a huddle leader • Establish key issues to be addressed • Provide the necessary training; retrain as needed • Recognize team members for contributions • Leader observations for effectiveness • Trend results and share with the team • Celebrate the prevention of patient harm 30 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 31 Wrap Up 1. Assess quality of patient care communications 2. Assess and determine need for safety culture shift 3. Select a consistent approach to hand offs and huddles 4. Educate teammates and practitioners 5. Implement posters, signage, other supports 6. Monitor effectiveness 7. Share the findings with the team 32 Agenda 1. Objectives 2. Review of ASC clinical outcomes trends 3. Role of communication in patient safety 4. Hand off communication 5. Huddles 6. Wrap up 7. Questions 33 Questions 34