Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
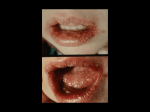
Passive Transfer of Anti-Herpes Simplex Virus Type 2 Monoclonal and Polyclonal Antibodies Protect Against Herpes Simplex Virus Type 1-Induced but Not Herpes Simplex Virus Type 2-Induced Stromal Keratitis Mary H. Ritchie, John E. Oakes, and Robert N. Lausch Purpose. To investigate whether passive transfer of antibodies to viral glycoproteins would protect against herpes simplex virus type 2-induced stromal keratitis. Methods. Balb/c mice were infected on the scarified cornea with herpes simplex virus types 1 or 2 (HSV-1 and HSV-2, respectively), and monoclonal or polyclonal antibodies were administered intraperitoneally 24 hr later. Eyes were monitored for corneal opacity. Flow cytometry was used to examine the expression of glycoproteins on the surface of HSV-infected cells. Results. Passive transfer of monoclonal antibodies to viral glycoproteins gB, gD, or gE or anti-HSV-2 hyperimmune serum were all highly effective (P < 0.005) at preventing blinding disease induced by HSV-1. In contrast, none of the antibody preparations could prevent stromal keratitis when the animals were challenged with various HSV-2 strains. However, antibody treatment could prevent the development of fatal encephalitis in the majority of HSV-2 infected hosts. Flow cytometry analysis revealed that gD and gB expression on the membranes of HSV-2 infected corneal epithelial cells isolated from excised corneas was substantially less (P < 0.005) than that detected on HSV-1 infected cells at both 24 and 48 hours postinfection. This antigenic difference was not due to the failure of HSV-2 to replicate in corneal epithelial cells in vivo. Conclusions. Decreased levels of membrane glycoprotein antigen expression may be one factor contributing to the refractiveness of HSV-2-induced ocular disease to humoral immunotherapy. Invest Ophthalmol Vis Sci. 1993; 34:2460-2468. Jrierpes simplex keratitis is the most common cause of corneal disease and the second leading cause of blindness in the United States.12 Although herpes simplex virus type 1 (HSV-1) has traditionally been associated with herpetic eye disease, herpes simplex virus type 2 (HSV-2) eye infections are becoming increas- From the Department of Microbiology and immunology, College of Medicine, University of South Alabama, Mobile, Alabama. Supported in part by grant N1H EY-07564. Submitted for publication: September I, 1992; accepted December 21, 1992. Proprietary interest category: N. Reprint requests: Robert N. Uiusch, Department of Microbiology and Immunology, College of Medicine, University of South Alabama, Mobile, AL 36688. 2460 ingly important in adults.3"8 Indeed, HSV-2 eye infections may manifest more severe and prolonged corneal lesions than those caused by HSV-1.67 The corneal opacification and scar formation that develop are at least partly attributable to the host immune response.9 HSV-1 inoculated onto the scarified cornea of Balb/c mice produces a blinding necrotizing stromal keratitis. Studies of HSV-1 murine corneal infection have indicated that this disease also has an immunopathologic basis.1011 That is, immune T cells responding to HSV-1 infection play a prominent role in the inflammatory process. To date the humoral immune Investigative Ophthalmology & Visual Science, July 1993, Vol. 34, No. 8 Copyright © Association for Research in Vision and Ophthalmology Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 2461 Antibody and HSV-2 Corneal Infection response has not been shown to contribute to the immunopathology. Instead, we1213 and others14'16 have found that the timely administration of monoclonal antibody to selected viral glycoproteins is highly effective at preventing the development of blinding corneal disease. Ten different glycoproteins have been identified on the virion surface and the plasma membrane of the infected host cell where they serve as targets of the immune response.1718 Glycoproteins gB and gD are among the most immunogenic and constitute candidates for a subunit vaccine.19"22 The genes of HSV-1 and HSV-2 display substantial homology, and so the glycoproteins of the two serotypes share numerous cross-reactive epitopes.2324 HSV-2 infection of the murine cornea also can induce stromal keratitis, which is clinically indistinguishable from that induced by HSV-1. However, it is not known whether antibody immunotherapy can prevent corneal disease induced by this serotype. To investigate this question experiments were conducted with a number of monoclonal antibodies to HSV glycoproteins, and also with hyperimmune serum. In contrast to our results with HSV-1, antibody failed to protect when HSV-2 was used as the challenge virus. Studies investigating possible reasons for the inability of antibody to promote resistance against HSV-2 corneal infection are described. MATERIALS AND METHODS Animals Three- to four-week-old female Balb/c mice were purchased from Charles River Breeding Laboratories (Wilmington) MA. The animals were treated and housed in accordance with the ARVO Resolution on the Use of Animals in Research. Viruses HSV-1 (17) and HSV-2(186) were originally obtained from Bernard Roizman (University of Chicago, Chicago, IL). HSV-1 (RE) was originally obtained from Ysolina Centifanto-Fitzgerald (Tulane University, New Orleans, LA), and HSV-2(333) was obtained from Fred Rapp (Hershey Medical Center, Hershey, PA). HSV-2(Av) was obtained from Richard J. Whitley (University of Alabama, Birmingham, AL). After being plaque-purified, virus stocks were grown in Vero cells and titrated by a plaque assay as previously described.25 Antibodies The anti-HSV glycoprotein D (gD) monoclonal antibody (mAb) 8D2 was prepared and purified as previously described.26 Anti-gD mAbs III-l 14-4 and III174-1.2 raised via immunization with HSV-2(G)27 were donated by Patricia G. Spear (Northwestern University Medical School, Chicago, IL). III-114-4 is of the IgG2b isotype whereas 8D2 and III-l 74-1.2 are IgG2a as determined by radial immunodiffusion (RID). AntigB (F3AB) and anti-gE (H7E), both IgG2a antibodies, were prepared as described by Rector et al.26 AntiHSV-2 hyperimmune mouse sera was raised via immunization with HSV-2(333). The dosages of antibody given were 200 /ig of III-l74-1.2 or III-l 14-4, a 1:2 dilution of a-HSV-2 serum, and 2000 /*g of F3AB and 500 ^ig of H7E. Antibodies were passively transferred by inoculating a 0.2 ml volume intraperitoneally. Corneal Infection Mice were anesthetized with 0.2 ml of sodium pentobarbital at a concentration of 5 mg/ml, and one eye was scarified by three twists of a 2 mm corneal trephine. A 2 fi\ volume containing the desired challenge dose of HSV was dropped onto the scarified cornea and rubbed in with the eyelids. Eye scores were read weekly using a dissecting biomicroscope with a fiber optic light source. Corneal opacity was graded on a scale of 0 to +5 as described by Metcalf et al.14 The person scoring the eyes was ignorant of the treatment the mice received. Isolation of Mouse Corneal Epithelial Cells Corneas from HSV infected and uninfected mice were excised and incubated in 5 mmol/1 ethylenediaminetetraacetic acid (EDTA) for 20 min in 5% carbon dioxide at 37°C. Using forceps the epithelial sheets were lifted off the stromal-endothelial portions of the cornea and incubated with 0.1% trypsin for 5 min in 5% carbon dioxide at 37°C. The epithelial sheets were then passed repeatedly through a 25-g needle to dissociate the cells. The cells were washed twice with buffer (phosphate buffered saline with 2% fetal bovine serum and 0.1% sodium azide) before being used in further tests. Fourteen to twenty epithelial sheets were pooled for each sample. Comparable numbers of epithelial cells were recovered from HSV-1- and HSV-2-infected corneas, and the percentage of cells recovered that were viable was > 80% for both serotypes. Fluorescence Activated Cell Sorter The reactivity of mAb with cultured mouse corneal fibroblasts or isolated corneal epithelial cells was analyzed by fluorescence activated cell sorter (FACS). Corneal fibroblasts were cultured as previously described.28 The cells (2X106) were seeded into 75 cm2 flasks and allowed to adhere overnight. The monolayers were infected with HSV-1 (RE) or HSV-2(333) at a multiplicity of infection of 3. After 45 min adsorption, fresh medium was added and the cells were incubated for various intervals. At the desired times postin- Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 2462 Investigative Ophthalmology & Visual Science, July 1993, Vol. 34, No. 8 fection the cells were harvested with trypsin/EDTA (0.25% trypsin, 1 mmol/1 EDTA-4Na, Gibco BRL, Grand Island, NY). The mouse corneal fibroblasts or epithelial cells were prepared for FACS analysis according to the protocol used by Jennings et al.29 The cells were washed twice with FACS buffer (phosphate buffered saline with 2% fetal bovine serum and 0.1% sodium azide) and underwent centrifugation. The resulting pellet was suspended at 1X106 viable cells/ml and 100 pi was separated into aliquot portions into wells of a 96-well plate. The cells were centrifugated and the supernatant was removed. The pellet was suspended with 50 ixl of primary antibody and incubated for 30 min at 4°C. The cells were washed with 150 n\ of FACS buffer containing an additional 27% fetal bovine serum. After centrifugation the supernatant was removed and the resulting pellet was suspended in 50 /xl of secondary antibody and incubated for 30 min at 4°C. The secondary antibody was fluorescein isothiocyanateconjugated goat anti-mouse affinity purified F(ab)'2 fragments (Cappell Research Products, Durham, NC). The cells were washed twice with FACS buffer and analyzed using an FACS 440 (Becton Dickinson, San Jose, CA). The mean fluorescence intensity (MFI) was calculated by using the formula: 2 (Number of cells in a channel)(channel number) Total number of cells analyzed HSV Growth in Mouse Corneal Cells Three to five corneas from mice infected with the desired concentration of HSV were excised at varying time points after infection, and the epithelial layers were separated from the stromal-endothelial layers as described earlier. After separation the samples from each cornea were frozen at —70°C. The samples were subsequently thawed, sonicated for 10-20 sec using a Sonic 300 Dismembrator (Arteck Systems Incorporated, Farmingdale, NY), and titrated for infectious virus by plaque assay on Vero cell monolayers. The infectious virus titer of infected isolated corneal epithelial cells was also determined from aliquot portions of the same samples used by FACS analysis. The corneal epithelial cells were isolated as described above. After being washed twice with FACS buffer, 5X104 cells per sample were dispersed into test tubes and frozen at —70°C. The samples were then thawed, sonicated, and assayed for infectious progeny on Vero cell monolayers. Statistical Analysis The Mann-Whitney U test was used to determine significant differences in the corneal opacity scores between control and test groups. Student's t test was used to compare the MFI values between HSV-l(RE)and HSV-2(333)-infected cells. RESULTS The reported AMFI values represent the MFI of the test samples minus the MFI of the IgG2a controls. 8D2 mAb Treatment Fails to Prevent HSV-2Induced Stromal Keratitis The mAb 8D2 recognizes a type common discontinuous epitope on gD and neutralizes HSV-2 strains TABLE l. Effect of Anti-gD Therapy on HSV-Induced Stromal Keratitis and Encephalitis* Challenge Virus HSV-1 (17) HSV-1 (17) HSV-2 (186) HSV-2 (186) HSV-2 (AV) HSV-2 (333) Viral Challenge Dose (PFU/eye) 2 X 105 2 X 105 4 X 104 4 X 1O4 2 X 105 2 X 1O5 4 X 104 4 X 104 4 X 104 4 X 104 4 X 104 4 X 104 8D2 MAb Treatment No. Survivors/ Total 6/6 3/6 6/6 5/6 6/6 6/6 6/6 6/6 4/6 0/6 7/7 6/7 Survivor Mean Corneal Opacity Score (P Value) 3 ° (<0.025) 0 (0.005) 4.4 4.8 (NS) 5.0 3.0 4.8 (NS) 5.0 4.8 (NS) 5.0 * Mice were infected on the trephined cornea with the indicated strain and challenge dose of HSV. Twenty-four hours after corneal infection, the animals were given MAb 8D2 (55 ^g) or control IgG2a (55 ng) intraperitoneally. Survivors are defined as those living at the time corneal opacity scores were determined. Corneas were examined on days 4 or 28 post-infection. NS = not significant. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 Antibody and HSV-2 Corneal Infection 2463 to the same high titer (103) as HSV-1 strains. Previous studies have shown that this purified antibody is strikingly effective at preventing or significantly reducing the incidence of HSV-1-induced stromal keratitis.12 We tested whether 8D2 would also protect mice challenged on the cornea with HSV-2. Table 1 shows that a dose of 55 jug/mouse, which provided excellent protection against HSV-1 strain 17 corneal infection, failed to protect animals infected with any of three different HSV-2 strains. Moreover, administering the antibody 30 min before HSV-2 corneal infection, or increasing the mAb dose to 110 ^,g/mouse, that is, tenfold higher than that shown to be effective against HSV-112, failed to provide protection against HSV-2 challenge (data not shown). It was possible that the failure to protect against stromal keratitis was peculiar to mAb 8D2. Therefore, an additional five mAbs that were specific for type common continuous epitopes or other discontinuous epitopes on gD were tested. None proved to be efficacious although allfivehad previously been shown to protect against HSV-1 strain RE corneal challenge13 (data not shown). 8.0 Q 4.0 ».O * O S § o D A • # o t.O r L. Q. «1.0 CO O QC UJ (0 D QC ••••—ooooo DAYS POST INFECTION FIGURE 2. Titers of HSV-1 and HSV-2 in corneal epithelial and stromal—endothelial layers. The right, corneas were infected with 4 X 104 plaque-forming units of HSV-1 strain 17 (•) or HSV-2 strain 333 (O) on day 0. At the indicated times after infection three tofivecorneas were excised. The epithelial layers were separated from the stromal-endothelial portions and each was titrated for infectious virus. Panel A (top) shows infectious virus titers of individual epithelial layers while Panel B (bottom) depicts the virus titers observed in the individual stromal-endothelial layers. w d O o CO o < Q. O < UJ Protection Studies with Other Monoclonal and Polyclonal Antibodies O O < UJ IgG2a a-gD' a-gD PBS a-HSV-2 IgG2a a-gB a-gE ANTIBODY TREATMENT l. Effect of mAb and hyperimmune serum therapy on HSV-induced stromal keratitis and encephalitis. Mice were infected on the trephined cornea with 4 X 104 plaqueforming units of HSV-1 strain RE (Panels A, B, C) or HSV-2 strain 333 (Panels D, E, F). The desired antibody was given intraperitoneally 24 hr later. Controls received an equivalent amount of IgG2a or phosphate buffered saline. There were initially 6-9 mice in each group. The opacity scores were determined on day 21 or 28 postinfection. Parentheses indicate the number of survivors per total number challenged. *P < 0.005, fcv-gD mAb Ill-l 14-4, Ja-gD mAb III174-1.2. FIGURE In the forgoing experiments all of the anti-gD mAbs tested had been produced in response to HSV-1 immunization. There are data that indicate that antibodies raised against HSV-2 may be more therapeutically active against HSV-2 than antibodies raised against HSV-1.30 Therefore, two anti-gD mAbs raised through immunization with HSV-2 were tested by passive transfer intraperitoneally 24 hr after infection. We found that antibodies III-l 14-4 and III-174-1.2, provided excellent protection against HSV-1 strain RE challenge (Figure 1A) but neither could protect against HSV-2 strain 333 (Figure ID) ocular infection. Similarly, a polyclonal hyperimmune mouse serum raised against HSV-2 and tested at a 1:2 dilution was therapeutically effective against HSV-1 (Figure IB) but not against HSV-2 (Figure IE). Additional protection studies were performed using type common mAbs to two other major glycopro- Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 Investigative Ophthalmology & Visual Science, July 1993, Vol. 34, No. 8 2464 tein antigens, gB and gE. Anti-gB and anti-gE were highly effective in protecting against HSV-1 challenge (Figure 1C) but failed to prevent corneal disease induced by HSV-2 infection (Figure IF). Conversely, Figure 1 (Panels D and F) also shows that 79% (27/34) of the niAb-treated hosts survived HSV-2 infection whereas only 12% (2/17) of the virus-infected controls did so. Thus,rnAbsto glycoproteins B, D, and E could provide significant (P < 0.05) protection against type 2-induced encephalitis. 10 3 io4 10° 10' 13h HSV-1 10° 101 10 2 10 3 10* 10° 10 1 10 2 10 3 10 4 10° 101 10 2 10 3 10* 10° 101 10 2 103 10* Log Fluorescence Intensity FIGURE 3. Cell surface expression of gD on HSV-infected cultured mouse corneal fibroblasts as analyzed by FACS. Monolayers of mouse corneal fibroblasts were infected with HSV-1 strain RE (Panels A and B) or HSV-2 strain 333 (Panels C and D) at a multiplicity of infection of 3 and harvested at the indicated times postinfection. The cells were stained with anti-gD mAb III32D174-1.2 (—) or an IgG2a control [g (—) followed by fluorescein isothiocyanate-conjugated goat anti-mouse affinity purified F(ab')2 fragments. The AMFI values are (A) 37, (B) 67, (C) 23, and (D) 45. io 3 io4 Day 2 HSV-2 HSV-1 and HSV-2 Growth in Murine Corneas Studies were initiated to determine why antibody failed to protect against HSV-2 induced stromal keratitis. One possibility was that HSV-2 replicated to higher titer in ocular tissue than HSV-1 and thereby overwhelmed the therapeutic effect of antibody. To investigate this hypothesis virus titers in epithelial (Figure 2A) and stromal-endothelial (Figure 2B) layers of individual corneas were determined at various times post infection. Although HSV-1 replicated to slightly higher titers than HSV-2 the differences were not statistically significant at any time point for either corneal layer. By day 7 postinfection only residual amounts of HSV-1 and HSV-2 were detected. Thus, HSV-2 was not found to replicate more extensively or persist longer in ocular tissue than HSV-1. io2 10* Log Fluorescence Intensity FIGURE 4. Cell surface expression of gD on epithelial cells isolated from HSV-infected mouse corneas as analyzed by FACS. Mice were infected on the scarified cornea with 1 X 106 plaque-forming units of HSV-1 strain RE (Panels A and B) or HSV-2 strain 333 (Panels C and D). The corneal epithelial cells were isolated at the indicated times postinfection and stained with anti-gD mAb III-l 74-1.2 (—) or an IgG2a control Ig (—) followed by fluorescein isothiocyanate-conjugated goat anti-mouse affinity purified F(ab')2 fragments. The AMFI values are (A) 23, (B) 21, (C) 5, and (D) 3. Glycoprotein Antigen Expression on HSVinfected Cell Membranes Because antibody was not administered until 24 hr after corneal infection the target in vivo was expected to be cell-associated virus antigen rather than cell-free virus. Perhaps less glycoprotein antigen was being expressed on the surface of HSV-2 infected cells compared to that found on HSV-1-infected cells. To address this possibility FACS analysis was performed using III-l 74-1.2, an anti-gD mAb generated by HSV-2 immunization. We first compared the levels of gD found on mouse corneal fibroblasts that had been grown in culture and then infected with HSV-1 or HSV-2. Glycoprotein antigen was readily detected on the surface of HSV-1 (Figure 3A and 3B) and HSV-2 (Figure 3C and 3D) infected cells at 8 and 13 hr postinfection. We next investigated whether the levels of gD on corneal epithelial cells were also comparable after corneal infection in vivo. Single-cell preparations derived from epithelial sheets of excised corneas were examined by FACS 1 and 2 days postinfection. As shown in Figure 4 (Panels A and B) gD was clearly demonstrable on the surface of HSV-1- infected cells at both time points. However, the results with HSV-2 were quite Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 2465 Antibody and HSV-2 Corneal Infection different. In Figure 4 (Panels C and D), little or no gD antigen could be seen. These results were consistently obtained in six independent experiments. Analogous studies were conducted to assess gB expression in vivo. Results representative of 5 independent experiments are shown in Figure 5. Although gB could be detected on HSV-2 infected cells (Figure 5C and D), the amount was consistently low and significantly less (P < 0.005) than that expressed on HSV-1infected cells (Figure 5A and B). HSV-1 and HSV-2 Titers in Isolated Corneal Epithelial Cells It was possible that the reduced HSV-2 glycoprotein expression observed in vivo reflected reduced HSV-2 replication in the epithelial cells analyzed. Therefore, aliquot portions of the same preparations used for FACS analysis were titrated for infectious virus content. The results of two such experiments are shown in Figure 6. It is evident that HSV-2 could readily replicate in mouse corneal epithelial cells although the titers tended to be approximately threefold lower than those for HSV-1. Whether the slightly lower virus yield was sufficient to account for the reduced gB and gD antigen expression on the surface of HSV-2-infected cells is not clear. 10' 10 10' 10 J 10' 10 u 101 10* 10' Log Fluorescence Intensity FIGURE 5. Cell surface expression of gB on epithelial cells isolated from HSV-infected mouse corneas as analyzed by FACS. Mice were infected on the scarified cornea with 1 X 106 plaque-forming units of HSV-1 strain RE (Panels A and B) or HSV-2 strain 333 (Panels C and D). The corneal epithelial cells were isolated at the indicated times postinfection and stained with anti-gD mAb F3AB (—) or an IgG2a control Ig (—) followed by fluorescein isothiocyanate-conjugated goat anti-mouse affinity purified F(ab')2 fragments. The AMFI values are (A) 21, (B) 17, (C) 8, and (D) 7. Exp. #2 Q| 4.0 1 2 3 1 2 DAYS POST INFECTION FIGURE 6. HSV-1 and HSV-2 titers in epithelial cells derived from infected mouse corneas. Mice were infected on the trephined cornea with 1 X 106 plaque-forming units of HSV-1 strain RE or HSV-2 strain 333. At the indicated times the corneas were excised, and the epithelial cells were isolated as described in the Materials and Methods section. The lysates from 5 X 104 cell aliquot portions were assayed for infectious progeny. DISCUSSION The major observation in this report is that passively transferred antibody failed to prevent stromal keratitis after HSV-2 corneal infection. This was the case regardless of whether the immunoglobulin transferred was anti-HSV-2 hyperimmune polyclonal serum or mAbs to gD, gB, or gE. Whether antibodies to other viral glycoproteins would be protective remains to be determined. However, it is striking that the same monoclonal and polyclonal antibody preparations that failed to protect against HSV-2 were highly effective in preventing corneal disease induced by HSV-1. It is important to emphasize that not all tissues infected by HSV-2 were unresponsive to antibody therapy. We found that immunoglobulin treatment consistently protected the majority of the recipients against viral encephalitis that developed as a consequence of HSV-2 spread into the central nervous system. This latter observation agrees with previously published reports. Thus, antibody transferred before31 or after32 HSV-2 footpad challenge was found to protect mice against fatal central nervous system disease. In addition, mAbs to gD33 as well as polyclonal HSV-2 specific antibodies34 have been shown to prevent skin and retinal lesions resulting from HSV-2 subcutaneous infections. McDermott et al35 reported that mice given antigC or anti-gD mAbs were protected against HSV-2 footpad but not intravaginal challenge. These authors suggested that antibody ineffectiveness against the latter was attributable to a lack of transudation into vaginal secretions. However, Eis-Hiibinger et al,36 found that antibody treatment readily protected mice inocu- Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 2466 Investigative Ophthalmology & Visual Science, July 1993, Vol. 34, No. 8 lated intravaginally with HSV-1. Thus, vaginal tissue may be a body site where antibody can protect against HSV-1 but not HSV-2 lethal infection. Collectively, our experiments in the cornea and those involving intravaginal infection suggest that the capacity of immunoglobulin to prevent disease is dependent on both the tissue infected and the infecting HSV serotype. There are a number of potential explanations for the failure of antibody to prevent HSV-2 corneal disease. One possibility is that HSV-2 replicated more rapidly and to a higher titer in ocular tissue than HSV1, thereby overwhelming the protective effect of antibody. We investigated this hypothesis and found that the two serotypes replicated to similar levels in corneal cells. In an earlier study in rabbits Stevens and Oh37 reported that HSV-2 titers in the eye were 100-fold lower than those of type 1. Thus, there is no evidence to support the theory that HSV-2 replicates more extensively in ocular tissue than HSV-1. Stevens and Oh37 also noted that corneal inflammation in rabbits infected with HSV-2 strains was more severe than in animals infected with HSV-1 strains. In our work blepharitis appeared to be more intense in the HSV-2-infected mice (unpublished observation). Recent studies in our laboratory have shown that interleukin la can be detected in HSV-1 infected murine corneal buttons, and that effective mAb immunotherapy is accompanied by decreased production of this pro-inflammatory cytokine38. One can speculate that the inflammatory cytokine cascade induced following HSV-2 infection differs either quantitatively or qualitatively from that induced by HSV-1 infection, and thus was insensitive to putative antibody-mediated down-regulation. A comparative analysis of cytokine expression after HSV-1 and HSV-2 infection merits investigation. Through FACS analysis we discovered a definite disparity in gD antigen expression between HSV-1 and HSV-2 infected cells after in vivo infection. Although gD was readily detected on epithelial cells isolated from HSV-1 infected corneas it was barely demonstrable on epithelial cells isolated from HSV-2 infected corneas. Moreover, surface gB was also more abundant on HSV-1 than HSV-2 infected cells. In contrast, the amount of surface gD was similar on cultured mouse corneal fibroblasts infected in vitro with HSV-1 or HSV-2. These results are compatible with the observations of Jennings et al.29 They reported that the kinetics and amount of glycoprotein antigen expressed on HSV-infected cells varied according to the host cell type. Reduced glycoprotein antigen expression on the surface of one target cell type but not another could conceivably explain why antibody treatment prevents HSV-2-induced central nervous system disease but not stromal keratitis. Likewise, a difference in glycoprotein expression could account for why antibody protects against HSV-1- but not HSV-2 induced corneal disease. Although we currently favor this explanation, our conclusions are strictly tentative because a causal relationship has not been established. To explain the dichotomy in corneal protection it will be important to develop an understanding of why antibody is effective against HSV-1 challenge. The failure to detect accelerated clearance of virus from ocular tissue of antibody-treated hosts12 suggests that conventional antibody protective mechanisms such as virus neutralization, or antibody-mediated lysis of infected cells, are not operative. A multiplicity of factors in addition to the extent of virus replication appear to influence how much viral glycoprotein antigen will be expressed by infected cells. Gething et al.39 have shown that the correct folding of the influenza virus hemagglutinin is required for it to be transported from the endoplasmic reticulum to the cell surface. Similar conclusions were reached by de Silva et al40 in studies on vesicular stomatitis virus G protein. Therefore, it is possible that HSV-2 glycoproteins fail to fold in a conformation that is conducive for efficient transport to the corneal epithelial cell surface. Johnson and Smiley41 observed that the kinetics of intracellular transport of gD in HSV-2 infected L cells was much slower than in transformed mouse L cells. They suggested that gD interaction with viral structural components retarded its movement to the cell surface. In our study, HSV-1 replicated at least as well as HSV-2, which suggests comparable levels of viral structural components within cells infected with either of the two serotypes. Thus, it seems unlikely that inhibition in gD transport would be greater in type 2- than type 1-infected cells. The kinetics of glycoprotein appearance on infected cell membranes as well as the amount made seems to be critical. Thus, Wachsman et al.42 have found that gD-1 expressed under the control of an early but not a late promoter in vaccinia recombinant viruses could protect guinea pigs from cutaneous HSV-2 disease. Regulation of glycoprotein genes during viral infection can occur at the levels of transcription43 and posttranscription.44 Several immediate early proteins including ICPO,45 ICP4,46-47 and ICP27 44 have been shown to play a role in regulating viral glycoprotein gene expression. Possibly the differential interaction of HSV-1 and HSV-2 immediate early gene products with components of the host cell could account for the dissimilarity in virus-infected cell surface glycoprotein expression in selected cell types. Alternatively, glycoproteins may be shed in greater abundance by HSV-2-infected cells into the corneal interstitium making it harder to eliminate stromal disease by passive immunization. In summary, we have shown that passive transfer of antibody fails to prevent HSV-2-induced stromal keratitis, although it provides excellent protection against HSV-1 ocular infection. However, antibody Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 Antibody and HSV-2 Corneal Infection therapy is able to prevent encephalitis induced by HSV-2 spread into the central nervous system. The dissimilar protection seen in different tissues suggests that the protective mechanism is influenced by inherent properties of the infected host cell as well as the genetic makeup of the infecting HSV serotype. Key Words 2467 14. 15. HSV-1, HSV-2, monoclonal antibodies, stromal keratitis, HSV glycoproteins 16. Acknowledgments The authors thank Ray Hester, PhD, for flow cytometry assistance and Nikki Nixon for manuscript preparation. References 1. Vaughan D. Viral keratitis. In: Vaughan D, Asbury T, Tabbara KF, eds. General Ophthalmology. Norwalk, CT: Appleton & Lange; 1989:104-125. 2. Whitley RJ. Herpes simplex virus. In: Fields BN, Knipe DM, et al, eds. Virology. New York: Raven Press; 1990:1843-1887. 3. Oh JO, Kimura SJ, Ostler HB. Acute ocular infection by type 2 herpes simplex virus in adults. Report of two cases. Arch Ophthalmol. 1975; 93:1127-1129. 4. Oh JO, Kimura SJ, Ostler HB, Dawson CR, Smolin G. Oculogenital transmission of type 2 herpes simplex virus in adults. Surv Ophthalmol. 1976; 21:106-109. 5. Hanna L, Ostler HB, Keshishyan H. Observed relationship between herpetic lesions and antigenic type of Herpesvirus hominis. Surv Ophthalmol. 1976; 21:110-114. 6. Neumann-Haefelin D, Sundmacher R, Wochnik G, Bablok B. Herpes simplex virus types 1 and 2 in ocular disease. Arch Ophthalmol. 1978; 96:64-69. 7. Sumers KD, SugarJ, Levine R. Endogenous dissemination of genital Herpesvirus hominis type 2 to the eye. Br J Ophthalmol. 1980;64:770-772. 8. Rosenwasser GOD, Greene WH. Simultaneous herpes simplex types 1 and 2 keratitis in acquired immunodeficiency syndrome. AmJ Ophthalmol. 1992; 113:102-103. 9. Pepose JS. Herpes simplex keratitis: Role of viral infection versus immune response. Surv Ophthalmol. 1991;35:345-352. 10. Doymaz MZ, Rouse BT. Herpetic stromal keratitis: An immunopathologic disease mediated by CD4+ T lymphocytes. Invest Ophthalmol Vis Sci. 1992; 33:21652173. 11. Hendricks RL, Tao MSP, Glorioso JC. Alterations in the antigenic structure of two major HSV-1 glycoproteins, gC and gB, influence immune regulation and susceptibility to murine herpes keratitis. j Immunol. 1989; 142:263-269. 12. Lausch RN, OakesJE, Metcalf JF, ScimecaJM, Smith LA, Robertson SM. Quantitation of purified monoclonal antibody needed to prevent HSV-1 induced stromal keratitis in mice. Curr Eye Res. 1989;8:499-506. 13. Lausch RN, Staats H, OakesJE, Cohen GH, Eisenberg RJ. Prevention of herpes keratitis by monoclonal 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. antibodies specific for discontinuous and continuous epitopes on glycoprotein D. Invest Ophthalmol Vis Sci. 1991;32:2735-2740. Metcalf JF, Koga J, Chatterjee S, Whitley RJ. Passive immunization with monoclonal antibodies against herpes simplex virus glycoproteins protects mice against herpetic ocular disease. Cuir Eye Res. 1987;6:173-177. Raizman MB, Foster CS. Passive transfer of anti-HSV1 IgG protects against stromal keratitis in mice. CurtEye Res. 1988; 7:823-829. Shimeld C, Hill TJ, Blyth WA, Easty DL. Passive immunization protects the mouse eye from damage after herpes simplex virus infection by limiting spread of virus in the nervous system. J Gen Virol. 1990; 71:681687. Hutchinson L, Browne H, Wargent V, et al. A novel herpes simplex virus glycoprotein, gL, forms a complex with glycoprotein H (gH) and affects normal folding and surface expression of gH. J Virol. 1992;66:224O-225O. Muggeridge MI, Roberts SR, Isola VJ, Cohen GH, Eisenberg RJ. Herpes simplex virus. In: van Regenmortel MHV, Neurath AR, eds. Immunochemistry of Viruses. Vol 2. Amsterdam: Elsevier; 1990:459-481. Berman PW, Gregory T, Crase D, Lasky LA. Protection from genital herpes simplex virus type 2 infection by vaccination with cloned type 1 glycoprotein D. Science. 1984;227:1490-1492. Cremer KJ, Mackett M, Wohenberg C, Notkins AL, Moss B. Vaccinia virus recombinant expressing herpes simplex virus type 1 glycoprotein D prevents latent herpes in mice. Science. 1985; 228:737-740. Bernstein DI, Frenkel LM, Bryson YJ, Myers MG. Antibody response to herpes simplex virus glycoproteins gB and gD. f Med Virol. 1990; 30:45-49. Stanberry LR, Bernstein DI, Burke RL, Pachl C, Myers MG. Vaccination with recombinant herpes simplex virus glycoproteins: protection against initial and recurrent genital herpes. J Infect Dis. 1987; 155:914920. Watson RJ. DNA sequence of the herpes simplex virus type 2 glycoprotein D gene. Gene. 1983; 26:307-312. Bzik DJ, Debroy C, Fox BA, Pederson NE, Person S. The nucleotide sequence of the gB glycoprotein gene of HSV-2 and comparison with the correspondinggene of HSV22D1. Virology. 1986; 155:322-333. Lausch RN, Kleinschrodt WR, Monteiro C. Resolution of HSV corneal infection in the absence of delayed-type hypersensitivity. Invest Ophthalmol Vis Sci. 1985;26:1509-1515. Rector JT, Lausch RN, OakesJE. Use of Monoclonal antibodies for analysis of antibody-dependent immunity to ocular herpes simplex virus type 1 infection. Infect Ivimun. 1982;38:168-174. Para MF, Parish ML, Noble AG, Spear PG. Potent neutralizing activity associated with anti-glycoprotein D specificity among monoclonal antibodies selected for binding to herpes simplex virions. / Virol. 1985;55:483-488. Lausch RN, Su Y-H, Ritchie M, Oakes JE. Evidence endogenous interferon production contributed to the Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017 2468 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. Investigative Ophthalmology & Visual Science, July 1993, Vol. 34, No. 8 lack of ocular virulence of an HSV intertypic recombinant. Curr Eye Res. 1991;10(suppl):39-45. Jennings SR, Lippe PA, Pauza KJ, Spear PG, Pereira L, Tevethia SS. Kinetics of expression of herpes simplex virus type 1-specific glycoprotein species on the surfaces of infected murine, simian, and human cells: flow cytometric analysis./ Virol. 1987;61:104-112. Brown ZA, Benedetti J, Ashley R, et al. Neonatal herpes simplex virus infection in relation to asymptomatic maternal infection at the time of labor. N EnglJ Med. 1991; 324:1247-1252. Balachandran N, Bacchetti S, Rawls WE. Protection against lethal challenge of BALB/c mice by passive transfer of monoclonal antibodies to five glycoproteins of herpes simplex virus type 2. Infect Ivimun. 1982;37:1132-1137. Oakes JE, Rosemond-Hornbeak H. Antibody-mediated recovery from subcutaneous herpes simplex type 2 infection. Infect Ivimun. 1978; 21:489-495. Inoue Y, Oh JO, Minasi P. Protective effect of antiglycoprotein D antibody on herpetic chorioretinitis in newborn rabbits. Cwr Eye Res. 1991; lO(suppl): 159— 165. Friedlaender RP, Oh JO, Minasi P, Ohashi Y. Protective effect of passive immunization on herpetic retinitis of newborn rabbits. Curr Eye Res. 1987;6:161—166. McDermott MR, Brais LJ, Evelegh MJ. Mucosal and systemic antiviral antibodies in mice inoculated intravaginally with herpes simplex virus type 2 . / Gen Virol. 1990;7l:1497-1504. Eis-Hubinger AM, Mohr K, Schneweis KE. Different mechanisms of protection by monoclonal and polyclonal antibodies during the course of herpes simplex virus infection. Intervirol. 1991 ;32:351-360. Stevens TR, Oh JO. Comparison of types 1 and 2 Herpesvirus hominis infection of rabbit eyes. II. Histopathologic and virologic studies. Arch Ophthalmol. 1973;90:477-480. Staats HF, Oakes JE, Lausch RN. Quantitation of interleukin 1 alpha in mouse corneal buttons after HSV- 39. 40. 41. 42. 43. 44. 45. 46. 47. 1 ocular infection with and without protective antibody therapy. Invest Ophthalmol Vis Sci. 1992;33:786. Gething M-J, McCammon K, Sambrook J. Expression of wild-type and mutant forms of influenza hemagglutinin: the role of folding in intracellular transport. Cell. 1986;46:939-950. de Silva AM, Balch WE, Helenius A. Quality control in the endoplasmic reticulum: folding and misfolding of vesicular stomatitis virus G protein in cells and in vitro. fCellBiol. 1990; 111:857-866. Johnson DC, Smiley JR. Intracellular transport of herpes simplex virus gD occurs more rapidly in uninfected cells than in infected cells./ Virol. 1985;54: 682-689. Wachsman M, Aurelian L, Smith CC, Perkus ME, Paoletti E. Regulation of expression of herpes simplex virus (HSV) glycoprotein D in vaccinia recombinants affects their ability to protect from cutaneous HSV-2 disease. / Infect Dis. 1989; 159:625-634. Smith IL, Sandri-Goldin RM. Evidence that transcriptional control is the major mechanism of regulation for the glycoprotein D gene in herpes simplex virus type 112Dinfected cells./ Virol. 1988;62:1474-1477. Smith IL, Hardwicke MA, Sandri-Goldin RM. Evidence that the herpes simplex virus immediate early protein ICP27 acts post-transcriptionally during infection to regulate gene expression. Virology. 1992; 186:74-86. Chen J, Zhu X, Silverstein S. Mutational analysis of the sequence encoding ICPO from herpes simplex virus type 1. Virology. 1991; 180:207-220. Arsenakis M, Campadelli-Fiume G, Roizman B. Regulation of glycoprotein D synthesis: does «4, the major regulatory protein of herpes simplex virus 1, regulate late genes both positively and negatively? / Virol. 1988;62:148-158. Tedder DG, Pizer LI. Role for DNA-protein interaction in activation of the herpes simplex virus glycoprotein D gene./ Virol. 1988;62:4661-4672. Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933174/ on 05/02/2017