Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Taura syndrome wikipedia , lookup
Hepatitis C wikipedia , lookup
Influenza A virus wikipedia , lookup
Neonatal infection wikipedia , lookup
Orthohantavirus wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Canine distemper wikipedia , lookup
Marburg virus disease wikipedia , lookup
Canine parvovirus wikipedia , lookup
Henipavirus wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
Hepatitis B wikipedia , lookup
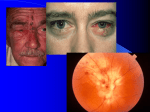
Micro Ch 41 Alpha Herpes Viruses: Herpes Simplex Viruses and Varicella-Zoster Virus Key Concepts Pathogen: Alpha herpes viruses: ds DNA viruses that include HSV types 1 & 2 and varicella-zoster virus (VZV) Encounter: high incidence of infection in humans; almost all people get HSV type 1; most asymptomatic Entry: HSV by direct contact; VSV from infectious aerosols Replication and Spread: establish latent infections following primary infection; latency makes it last for life and can lead to reactivation of virus replication and recurrent outbreaks Damage: HSV’s cause oral and genital herpes (occasionally encephalitis); VZV causes chickenpox and shingles Treatment: alpha herpes viruses treated w/antiviral agents (acyclovir); antiviral therapy doesn’t prevent future Prevention: VZV vaccines available for chickenpox and shingles Encounter HSV-1 spread by exchanging saliva; nearly 2/3 of adults have antibodies to HSV-1 HSV-2 acquired by oral-oral and oral-genital contact; primarily spread by genital-genital contact o 1/5 of all adults infected w/HSV-2, depending on nature and number of sexual encounters HSV-1 or HSV-2 cause severe disease in neonates if exposed during birth to mother w/primary infection VZV usually acquired through respiratory route; contact w/vesicular fluid or secretions can occur; primary disease much more contagious than HSV-1 and HSV-2 because direct contact not required o Breakthrough disease – mild form of chickenpox occurring in vaccinated pts; can transmit virus Most infections w/HSV-1 or HSV-2 asymptomatic; can still transmit virus by shedding from epithelial surfaces even if lesions not large enough to be noticeable Entry Membrane envelop causes them to be fragile and susceptible to drying and inactivation by heat, mild detergent, and solvents; infection usually requires direct contact Thick keratin layer of superficial epidermis prevents HSV from getting to receptors; mucous membranes not so strong barrier, so they get in here Spread and Replication Infection begins w/attachment of virus particles to susceptible cells; bind to cells through interaction of glycoproteins w/heparan sulfate chains on cell-surface; binding brings virus into close proximity to other cellsurface molecules that function as entry receptors o HSV-1 & HSV-2 preferentially use different receptors to infect different cell types at various portals of entry and in brain o Binding of viral glycoprotein to entry receptor triggers fusion of virion envelope and PM (or membrane of endosome); causes release of viral nucleocapsid into cytoplasm o Transport of nucleocapsid to nuclear pores; viral genome released into nucleus o In cell capable of supporting virus replication, virus genes transcribed in temporal fashion o If cell latently infected, viral genome circularizes in nucleus and persists as episome w/minimal transcription of viral genes o Virus gains access to nerve cell endings that extend toward epidermis and is transported to nerve cell bodies in peripheral sensory and autonomic ganglia, where latent infections established Productive infection: infection where virus replication occurs; immediate-early genes transcribed w/assistance of transcription factors carried in virion tegument (space between nucleocapsid surface and envelope) o Proteins encoded by immediate-early genes activate expression of early genes (protein products required to replicate viral DNA) o Late genes expressed after DNA synthesis; encode proteins that assemble and comprise progeny virions Glycoproteins insert into cell membranes As new viral nucleocapsids assembled in nucleus, they bud through inner nuclear membrane to acquire temporary envelope, which they lose by fusing w/outer nuclear membrane Final viral envelope w/full set of viral glycoproteins acquired by budding into cytoplasmic vacuoles derived from Golgi apparatus; vacuoles transport mature virions to surface for release by exocytosis As herpes viruses released from host cell, they immediately attach to and penetrate adjacent cells; diseases characterized by local spread and progression of lesions; HSV rarely spreads systemically o VZV causes systemic disease because of capacity to infect and be transported by circulating WBCs that deliver virus to multiple organs and skin by cell-to-cell contact Host Defenses Can prevent Sx in HSV-1 and HSV-2, but can’t prevent latent infections and can’t eliminate latent virus (latently infected cells don’t trigger sterilizing immune responses) Antibodies and T cells responsive to viral antigens o Anti-herpes virus antibodies play minor role in recovery from primary HSV or VZV because they develop too late to modify course of infection; no impact on recurrent disease either o Antibodies contribute to prevention of primary disease Cell-mediated immune mechanisms most important for recovery from HSV or VZV o Relevant immune effector cells gradually mature during first month of infant’s life; until maturation complete, herpes infections would be devastating; by 1 month of age, infection well-tolerated o Reactivation of VZV leading to zoster occurs w/increasing frequency as function of age (senescence of antiviral immune responses) Damage HSV and VZV destroy epithelial cells in which they replicate in skin and mucous membranes, causing vesicular lesions that rupture, leaving shallow gray-white ulcers on erythematous base o As virus replication and spread contained by immune responses (primarily innate and cell-mediated responses), epithelium fully regenerates Primary and recurrent HSV lesions usually localized (spread of virus restricted to regional nerves) o During primary disease, sequential lesions resulting from reseeding of adjacent epithelial sites by neurons infected during earlier waves of epithelial replication o Damage or inflammation of nerves causes itching, tingling, burning, or pain; similar sensations are prodrome that recurrent lesions about to develop o Reactivation of latent HSV by sunburn, systemic infections, immune impairment, emotional stress, and menstruation o Reactivated HSV travels down axonal processes to infect contiguous mucocutaneous epithelial cells Site of HSV inoculation governs manifestations of primary and recurrent disease o Corneal infections: immune responses that damage cornea; may cause blindness needing corneal transplant for recovery of vision o Primary genital herpes (HSV-2) can progress to meningitis or affect autonomic functions governing urination and defecation o HSV-1 can pass from peripheral nerves to CNS to cause encephalitis (destructive inflammation of unilateral focal nature) Accounts fo 95% of all cases of sporadic disease in children and adults in developed countries o Immunocompromised at risk for infections of skin, lungs, esophagus, liver, and brain VZV chickenpox: systemic febrile disease w/mucocutaneous lesions; cells of lymphatic system infected in respiratory tract; spread of virus-infected WBCs throughout lymphatic system induces types of cytokine responses that result in fever, malaise, and headache o Secondary viremia – circulating WBCs transmit virus to epithelial cells of skin and mucosa; characteristic lesions of chickenpox occur o Latent infections established in peripheral ganglia o Complications: cerebellar ataxia in otherwise healthy children and encephalitis in immunocompromised Zoster lesions (shingles) – appear clustered on body surface along dermatome o Neurological Sx (primarily pain) much more severe than for HSV recurrences (more viral damage to affected nerves and supporting cells) o Can cause severe disseminated disease in immunocompromised Diagnosis Presentation w/history usually sufficient Scrapings from lesions processed for PCR w/probes for viral DNA or stained directly w/specific fluoresceinlabeled antibodies that bind viral antigens Definitive diagnostic is virus isolation from cell culture; HSV grows well in wide variety of fibroblast and epithelial cell lines from animals or humans o Replicating viruses induce changes in cell shape and appearance o VZV more difficult to propagate in culture; more fastidious about cell type Treatment Acyclovir – analog for guanosine; phosphorylated by herpes virus enzymes but not cell enzymes; incorporated into viral DNA as chain-terminating nucleotide; active principally in herpes-infected cells Pencipclovir – guanosine analog used topically; poor oral bioavailability Valacyclovir – prodrug of acyclovir; improved oral bioavailability; treatment of either HSV or VZV Famciclovir – prodrug of penciclovir; improved oral bioavailability; treatment of either HSV or VZV Drugs may be administered IV or PO, depending on condition being treated Prevent worst of disease, but don’t effect cure because they don’t prevent entry of virus into neurons and can’t eliminate latent viral genomes Prevention Appropriate to avoid sexual contact during active genital herpes infections; reduces, not prevents, transmission Pts w/chickenpox should be isolated and vaccination offered to family members or other contacts o Exposed immunodeficient children not candidates for vaccination; protected by administration of specific human Ig promptly after exposure o Live, attenuated VZV vaccine prevents chickenpox in normal and some immunocompromised children Vaccine virus establishes latent infection; reactivation may lead to mild cases of shingles o New formulation boosts anti-VZV cellular immunity in older people and protects from shingles o Isolate patients w/primary VZV because virus can be transmitted via aerosols People w/active herpetic lesions shouldn’t be allowed contact w/newborn infants