Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Common cold wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Infection control wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Transmission (medicine) wikipedia , lookup
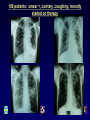
Theory of Airborne Infections Transmission Control Interventions Impact of Treatment Edward A. Nardell, MD Associate Professor Harvard Medical School Harvard School of Public Health Hospitals as Causes of Human Suffering Referring to the Hotel-Dieu in Paris which had a mortality rate of 1 in 4 patients “A fragment of space closed on itself, a place of internment of men and disease, its ceremonious but inept architecture multiplying the ills of its interior without preventing their outward diffusion, the hospital is more of a centre of death (foyer de mort) for the cities where it is sited, than a therapeutic agent for the population as a whole” Ref: Medicine and Magnificence – British Hospital and Asylum Architecture, 1660 – 1815, by Christine Stevenson, Yale University Press, 2000, page 155 Florence Nightingale 1820-1910 “Notes on Hospital Design 1859” Airborne infections as a buildingassociated illnesses Hospitals, clinics, laboratories Other indoor environments Prisons, jails, homeless shelters, residential facilities refugee camps, crowded outdoor environments transportation safety: Airliner, shipboard transmission Pine Street Inn 1984 TB Outbreak INH & SM res Shelter Transmission Exogenous Reinfection UVGI Air Disinfection Air Filtration Many other Interventions TB Resurgence - NYC (1985-92) TB Case Treatment barriers MDR TB Cure 50% Transmission Shelters, Jails, Hospitals HIV + HIV - 5 - 10% / year 5 - 10 % / lifetime Tuberculosis in New York City-turning the tide Frieden, T. R., Fujiwara, P. I., Washko, R. M., Hamburg, M. A N Engl J Med, 1995, 333:229-33 • “Epidemiologic patterns strongly suggest that the decrease in cases resulted from an interruption in the ongoing spread of M. tuberculosis infection, primarily because of better rates of completion of treatment and expanded use of directly observed therapy. • Another contributing factor may have been efforts to reduce the spread of tuberculosis in institutional settings, such as hospitals, shelters, and jails.” Global MDR-TB Treatment Scale Up • Estimated 500,000 new MDR-TB cases per year – More than half result from transmission – 2008 - 29,423 cases reported • 7% of estimated cases • 1% treated with quality assured drugs • Most are treated in hospitals for first 6 months – until culture conversion Source: Multidrug and extensively drug-resistant TB (M/XDR-TB) 2010 GLOBAL REPORT ON SURVEILLANCE AND RESPONSE Transmission: Hospitals as MDR TB Factories Tomsk, Siberia Glemanova, et al., Bull WHO, 2007; 85:703-711. • Studied the role of non-adherence and default on the acquisition of multidrug resistance • Substance abuse was NOT associated with MDR-TB • MDR-TB occurred among adherent patients who had been hospitalized, – Odds Ratio: 6.34 for hospitalized vs. patients treated as outpatients. Patients admitted with drug susceptible TB - Reinfected with MDR TB Anton Chekhov, MD Short story writer - Disliked Tomsk and Tomsk disliked him! - Died of TB TB IC Hierarchy • Administrative controls – Said to be most effective, least expensive – “FAST” – Barrera and Nardell. Int J. Tuberc Lung Dis, April, 2015 • Environmental controls* – Require less cooperation • Respiratory protection – Last intervention, not against unsuspected case TB transmission, c. 1930 Richard L. Riley & William F. Wells Wells’ Air Centrifuge, 1931 “On Airborne Infection, Study II. Droplets and Droplet Nuclei” W. F. Wells*. Am J Hygiene, 1934:20. 611-18. *Instructor, Sanitary Service, HSPH In 1931 Wells developed his air centrifuge to sample bacteria from air Droplet vs. Airborne spread Transmission within a meter of the source Relatively large numbers of organisms in inoculum (small incoculum may be tolerated) Access to vulnerable site (mucosal membranes of eye, nose, mouth, trachea, etc.) Hand washing may be effective Transmission beyond a meter – shared breathing volume Relatively small numbers of organisms in inoculum – virulence required Access to vulnerable site – alveoli in the case of TB Hand washing not effective. Strobe photo of cough/sneeze Particle size* & suspension in air Particle size & deposition site Time to fall the height of a room 100 20 10 – upper airway 1 - 5 – alveolar deposition *NOT organism size 10 sec 4 min 17 min Suspended indefinitely by room air currents Fate of aerosolized TB 10% survive aerosolization of those, 50% (5%) survive 6 hrs. (Loudon) if inhaled, only 0.25 to 50% (2.5%) lodge in the lung Particle deposition: Upper and lower respiratory tract TB is an infection of the alveolar macrophage Airborne infection requirements Pathogen must be dispersed as fine particles (1 – 5 um size) Remain suspended in air Reach the alveolar level (TB) Respiratory tract – cough aerosol TB wound – water pik Resistant upper respiratory tract Minute infectious dose (droplet nucleus) Upper room UVGI effect on measles in day schools, (Wells, Am J Hygiene, 35:97-121, 1942) Wells/Riley Experimental TB Ward Quantitative air sampling for TB Riley RL, Mills C, Nyka W. Aerial dissemination of tuberculosis – a two year study of contagion on a tuberculosis ward. Am J Hyg 1959; 70:185-196. Riley RL. What nobody needs to know about airborne infection. (How It Really Happened) AJRCCM 2001; 163:7-8. Infectivity of ward air 63 infectious particles (120 GPs x 8 cf per day x 730 days) = 1 infectious particle/11,000 cf High enough to explain infection rate of nurses Avg. 30 infectious particles added per day (1.25/hr) but the laryngeal case generated 60/hr Other, epidemiologic investigations have estimated 13 – 240/hr Example: TB Hospital outbreak recovery room Propagation of Mycobacterium tuberculosis Environmental Factors Room volume Room ventilation Temperature and humidity Aerobiology Environmental stresses: oxygen radiation Organism Take off Treatment Source viability drug resistance strength disease Landing number Virulence Host resistance Pathogenesis infection Airborne Infection - Interventions Temperature and humidity Aerobiology Environmental stresses: oxygen radiation Organism Take off Masks on patients Source Landing number Treatment viability Virulence drug resistance Host strength Immunization Resp Protection resistance Admin. Controls disease Dilution Filtration UVGI Isolation Pathogenesis infection Treatment of latent infection Mechanical Ventilation – theoretical limits of protection Nardell EA, et. al. Am Rev Resp Dis 1991; 144:302-6 27/67 (40%) office workers infected over 30 days 1st 1 secondary case Poor ventilation air change removes 63%, 2nd removes 63% of what is left, etc. Double ventilation = reduce risk by half, and so on…. 120 100 15 cfm/person 80 p 30 cfm/person 60 40 20 0 0 2000 4000 6000 Ventilation, CFM 8000 Building Usage Population density and distribution as a TB risk factor Large facility:1. higher probability of infectious cases 2. more people exposed 10 Small facilities 2% risk = 98 exposed Same 2% risk = 18 exposed, Now 80 protected = 82% risk reduction!! Does the Building Matter? Annual Risk of Infection Among Medical Students of Universidad Peruana Cayetano Heredia in Lima, Peru, ATS, May 20, 2002, Accinelli, Alvarez and colleagues. A A B • • 488 students Pos. PPD increased from 3.5% to 45.9% over 7 years • 6%/yr. avg. B How Effective are Surgical Masks on Patients? Respirators For patients For health care workers How Effective Are Surgical Masks on Patients? Guinea Pig Gro up TST 0 TST 1 TST 2 TST 3 TST 4 Total Intervent ion 0 1 10 20 5 36 Control 0 4 15 39 11 69 Approx 53% Effective Dharmadhikari AS, et. al. Am J Respir Crit Care Med. 2012 May 15;185(10):1104-9. NIOSH funded Slides courtesy of Dr. Norbert Ndjeka, Director, Drug Resistance and TB and HIV, MOH, South 32 Africa Province Registered Patients (08) Available Beds Variance (Beds-Pts) EC 797 394 -403 FS 265 75 -190 GP 601 266 -335 KZN 1,061 528 -533 LP 104 50 -54 MP 272 36 -236 NC 148 65 -83 NW 159 77 -82 WC 1,145 363 -782 RSA 4,552 1,824 -2728 2010 – Durban, South Africa National TB Conference 33 Community Based Treatment • Highly effective • e.g., Peru, Lesotho, Cambodia, KZN, and others • Less opportunity for institutional transmission But, what about community transmission? Effects of Chemotherapy on Transmission – Early Papers • • • • • • Andrews RH. Bull WHO. 1960 (Madras, India) Crofton J. Bull IUAT. 1962 (Edinburg, Scotland) Brooks S. Am Rev Resp Dis. 1973 (Ohio) Riley R. Am Rev Resp Dis. 1974 (Baltimore) Gunnels J. Am Rev Resp Dis. 1974 (Arkansas) Rouillon A. Tubercle. 1976 (Review): – Smear and culture correlate with infectivity only in untreated cases • Discordance between effect of treatment on culture and smear – Evidence that smear and culture positive TB patients on therapy do not infect skin test negative close contacts. • Menzies R. Effect of treatment on contagiousness of patients with active pulmonary tuberculosis. Infect Control Hops Epidemiol 1997; 18:582-586 The Madras Experience (Bull WHO 1966; 34:517-32) • The first clinical trials of ambulatory TB treatment demonstrated no more household conversions after the start of treatment – Most household contacts had been exposed for months before diagnosis and treatment – Susceptible contacts already infected – Patients no longer infectious Effects of Chemotherapy on Transmission • Riley and Moodie (ARRD, 1974): – studied 70 household contacts of 65 new TB cases on domiciliary treatment (non-RIF regimen) – never hospitalized. – A series of 6 TST results showed no transmission among 25 TST negative contacts after the start of treatment. – Most household contacts were infected in the month or two before diagnosis and treatment . Effects of Chemotherapy on Transmission • Gunnels et al (ARRD 1974): – studied contacts of 155 patients sent home after 1 month of treatment in hospital – 69 Culture neg. – 86 Culture pos • 52 Smear and culture positive. • No difference in infection rate among 284 contacts of culture pos cases versus 216 contacts of culture negative contacts Effects of Chemotherapy on Transmission • Rouillon A, Perdrizet S, Parrot R. Transmission of tubercle bacilli: The effects of chemotherapy. Tubercle 1976; 57:279-299. – Sputum smear and culture positivity correlate with transmission before but not on therapy • Discordance between effect of treatment on culture and smear – Evidence that smear and culture positive TB patients on therapy do not infect close contacts. Effects of Chemotherapy on Transmission (Rouillon) • “There is an ever-increasing amount of evidence in support of the idea that abolition of the patient’s infectiousness – a different matter from ‘cure,’ which takes months, and from negative results of bacteriological examinations, direct and culture, which may take weeks – is very probably obtained after less than 2 weeks of treatment”. • “These facts seem to indicate very rapid and powerful action by the drugs on infectivity…” CDC/ATS Policy on Treatment in general hospitals, communities, and discharge • 1969 ATS – Guidelines for the general hospital for the admission and care of tuberculosis patients. • 1970 ATS – Bacteriologic standards for discharge of patients • 1973 ATS – Guidelines for work for patients with tuberculosis • 1974 CDC – Recommendation for health department supervision of tuberculosis patients Riley Experimental TB Ward, 1956-60 Am J Hyg 1959; 70:185-196. (reprinted as “classic” Am J Epidemiol 1995; 142:3-14) Hundreds of sentinel guinea pigs sampled the air from a 6-bed TB ward in Baltimore TB transmission only from untreated patients - 1 • Patients selected: – strongly smear positive – cavitary TB • 3 of 77 patients produced 35 of 48 (73%) of GP infections that were cultured – all drug resistant M. tuberculosis on inadequate therapy – 4 month period of no infections when drug susceptible patients were admitted to the ward and started on treatment the same day 4 months Riley Ward – 2nd 2-year study - included untreated patients Relative infectivity of patients*: – Susceptible TB • 61 Untreated • 29 Treated (29 GPs) (1 GP) 100% 2% (14 GPs) (6 GPs) 28% 5% – Drug-resistant TB • 6 Untreated • 11 Treated *all smear positive patients, relative to the amount of time on the ward Riley’s conclusions ARRD 1962; 85:511-525 “The treated patients were admitted to the ward at the time treatment was initiated and were generally removed before the sputum became completely negative. Hence the decrease in infectiousness preceded the elimination of the organisms from the sputum, indicating that the effect was prompt as well as striking.” “Drug therapy appeared to be effective in reducing the infectivity of patients with drug resistant (H, SM, PAS only) organisms, but the data do not permit detailed analysis of the problem”. TB transmission only from untreated patients – Peru Escombe 2008 Plos Medicine; 5:e188 – 97 HIV+ pulmonary TB patients exposed 292 guinea pigs over 505 days • 66 cult +, 35 smear + – 122/125 GP infections (98%) were due to 9 MDR patients • all inadequately or delayed treatment » 108/125 infections (86%) due to 1 MDR patient • 3 drug susceptible patients infected 1 guinea pig each » 2 had delayed treatment » 1 had treatment stopped Dramatic Increase in antibiotic concentration as respiratory droplets evaporate into droplet nuclei Ref. Loudon, et al. Am Rev Resp Dis 1969; 100:172-176. Droplet Drug Concentration Airborne Evaporation Droplet Nucleus Sputum culture vs. GP Infection • • • Sputum sample – no evaporation – no aerosol damage No host defenses Growth support optimized Smear and culture positive • • • Droplet nucleus – evaporation with rising drug concentration – aerosol damage Host defenses Innate immunity No guinea pig infection How effective is treatment in stopping MDR-TB transmission? The AIR Facility Witbank, Mpumalanga Provence, RSA 109 patients: smear +, cavitary, coughing, recently started on therapy Guinea Pig Transmission: South Africa 109 patients: smear +, cavitary, coughing, recently started on therapy # Patients/ Exp. Duration % guinea pigs infected (# exposed) Patients # XDR (MGIT) Pilot 26* / 4 mos 74% (360) 3/11 Exp 1 24 / 3 mos 10% (90) 5/10 Exp 2 15 / 2 mos 53% (90) 2/11 Exp 3 27 / 3 mos 1% (90) 0/21 0/27 (LPA) Exp 4 17/ 3 mos 77% (90) 2/10 * 8 different spoligotypes, but only 2 transmitted to GPs – both XDR-associated Unsuspected, untreated TB TB DR General Medical Ward Orthopedic Ward Obstetrics Ward Psychiatric Ward TB DS Unsuspected, untreated MDR/XDR TB All other patients on effective treatment TB TB TB TB TB DR TB Hospital TB TB TB Potential for re-infection TB TB TB DR TB TB TB TB Triage – Rapid DR Diagnosis Smear status may not be critical if on effective treatment Individual Isolation XDR by LPA Effect of treatment unknown Novel interventions Gene Xpert: TB, DS or MDR Community based – on effective treatment – responding Complications Hospitalized patients on effective treatment - responding TB CARE Transmission Control Campaign: “F-A-S-T” • Find TB cases - rapid diagnosis • Focus on rapid molecular diagnosis – Xpert TB • Sputum smear – can also be rapid, but more limited • Active case finding • Focus on cough surveillance at all entrance points • Separate safely and reduce exposure • Building design and engineering • Cough hygiene and triage • Treat effectively, based on rapid DST • Focus on rapid molecular DST – Xpert TB FAST : Underlying Principles: 1. Most TB transmission is NOT due to known or suspected patients on effective therapy – Much of TB IC focuses on known and suspected cases, isolation /separation, air disinfection, respiratory protection, and sputum conversion. 2. Rapid identification of unsuspected TB cases and unsuspected drug resistance are top priorities 3. Effective treatment rapidly stops TB transmission regardless of sputum smear status. Not new, but never prioritized: Traditional TB IC F-A-S-T Strategy • • • • • • • Facility assessment Develop a TB IC plan Political will and resources TB IC committee WHO TB IC Policy – Administrative – Environmental – Respiratory protection Assessment – Process indicators – HCW cases • • • Risk of undiagnosed TB and undiagnosed DR TB Approach: F-A-S-T Political will and resources Focus on certain administrative components – – – – • Rapid diagnosis Active case finding Exposure reduction Effective treatment Assessment – Process indicators – HCW cases USAID F-A-S-T Implementation Project Ndola District, Zambia Ndola Central District Hospital Casualty Filter ward: Cough Surveillance OPD High Cost Clinic NCDH Clinics: Cough surveillance And treatment Lab: Xpert TB (2 hr dx TB and RMP resistance) RX – effective treatment -> no transmission Process indicators: 1.Time from cough onset to detection 2.Time from cough detection to sputum smear or Xpert TB test 3. Time from sputum receipt to result 4. Time from result to effective treatment. Twapia Clinic AFB Smear Lab And treatment Early FAST Results, National Institute of Diseases of the Chest, Dhaka, Bangladesh Preliminary Results on the FAST Strategy at NIDCH* Disease Category Total Samples Tested Number of Unsuspected TB Cases Identified (%) Number of Unsuspected MDR-TB Cases Identified (%) Current TB disease 42 Other respiratory disease with previous TB history 169 40 (23.66) 3 (1.77) Other respiratory disease 850 80 (9.41) 6 (0.70) Total 1062 120 (11.29) 12 (1.12) *Data reflect 11 weeks of implementation, starting February 2014. 3 (7.12) Conclusions • Airborne transmission may be the weak link in TB propagation – Only about 1/3 of pulmonary TB patients infect close contacts • Very little effective treatment may tip the balance against transmission • Sputum smear positivity correlates with infectiousness only in inadequately treated patients. • Strong rationale for prompt diagnosis of drug resistance and prompt effective therapy – can be in the community Continuing Communication Global Health Delivery On Line www.GHDonline.org GHDonline/infection control An on-line community of best practice Free, interactive Resource for documents, including these talks On line discussion Future uses: List consultants and contact information List contacts for past consultations