Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hemodynamics wikipedia , lookup
High-altitude adaptation in humans wikipedia , lookup
Cushing reflex wikipedia , lookup
Alveolar macrophage wikipedia , lookup
Human vestigiality wikipedia , lookup
Freediving blackout wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Haemodynamic response wikipedia , lookup
Cardiac output wikipedia , lookup
Common raven physiology wikipedia , lookup
Intracranial pressure wikipedia , lookup
Sleep apnea wikipedia , lookup
Obstructive sleep apnea wikipedia , lookup
Pre-Bötzinger complex wikipedia , lookup
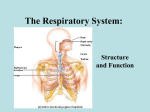
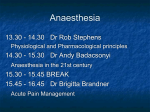
Respiratory physiology and anaesthesia Gary H Mills BMedSci MBChB FRCA Anaesthesia affects all aspects of respiratory system function. This can be considered in terms of effects on the control of breathing, chemoreceptors, upper airway, respiratory muscles and lung mechanics (including lung volume and airway resistance) and the impact these factors have on ventilation and perfusion. Control of breathing Anaesthetic agents influence rate, rhythm and intensity of discharge from the respiratory centres which receive input from the chemoreceptors, cortex, hypothalamus, pharyngeal mechanoreceptors, vagus nerve and other afferents. The respiratory centres are located in the pons and the medulla. These contain many different types of inspiratory and expiratory neurons that fire during the three phases of the respiratory cycle: Inspiratory phase: A sudden onset is followed by a ramp increase in discharge to the inspiratory muscles and the dilator muscles of the pharynx. Post-inspiratory phase: A gradual decline of discharge to the inspiratory muscles leads to a gradual reduction in tone which modulates expiratory flow. Expiratory phase: Both expiratory and inspiratory muscles are silent unless forced expiration or high minute ventilation (>40 l min–1) is required. The medulla contains cells that discharge rhythmically, including the dorsal and ventral groups of respiratory neurons. The dorsal area lies close to the tractus solitarius and mainly discharges on inspiration. The ventral area also contains some inspiratory neurons, i.e. the nucleus paraambiguus (controls force of inspiration) and the nucleus ambiguus (dilates the upper airway). However, most cells are expira- tory, including the expiratory Botzinger complex and the nucleus retroambigualis. The pons has a lesser role, adjusting the fine control of the respiratory rhythm, including setting the volume at which inspiration is terminated. Upper motor neurons from the respiratory centres pass via the ventrolateral part of the cord to the anterior horn cells. Their effect is combined with voluntary inputs that pass via the ventrolateral and dorsolateral cord, as well as involuntary inputs such as coughing and swallowing. Tension in the respiratory muscles is adjusted by the muscle spindles which are present in small numbers in the diaphragm. The effect of anaesthetic agents on respiratory drive Most inhalational anaesthetic agents increase respiratory frequency by shortening inspiratory and to a larger extent expiratory time. Tidal volume is depressed, as is ventilatory response to PaCO2. There is active contraction of the abdominal muscles during expiration and there may be paradoxical inward movement of the ribcage in early inspiration. Each anaesthetic agent has a slightly different effect on inspiratory and expiratory time and tidal volume. Ether has little effect on PaCO2 at low concentrations and nitrous oxide is not generally depressant. The response to hypoxaemia may be diminished by very low concentrations of volatile agents, but the degree of depression is a matter of debate. This effect is produced by action on the respiratory centre rather than a slight effect on peripheral chemoreceptors. If obstruction of the airway occurs during anaesthesia, pressures produced by the respiratory muscles in response to the obstruction are well preserved and are comparable to the awake state. Current intravenous induction agents produce a brief stimulation on induction which British Journal of Anaesthesia | CEPD Reviews | Volume 1 Number 2 2001 © The Board of Management and Trustees of the British Journal of Anaesthesia 2001 Key points Observation of respiration in the undisturbed patient has great value after anaesthesia After anaesthesia, decreased upper airway tone allows obstruction at less negative airway pressures Anaesthesia reduces chest wall and diaphragm tone causing functional residual capacity to fall rapidly to or below closing volume Ventilation perfusion mismatch is increased by anaesthesia during spontaneous breathing and intermittent positive pressure ventilation Respiratory complications and mortality are reduced by regional anaesthesia Gary H Mills BMedSci MBChB FRCA Honorary Consultant Anaesthetist and Senior Lecturer in Anaesthesia and Intensive Care Medicine, Section of Anaesthesia, Department of Surgical and Anaesthetic Sciences, K Floor, Royal Hallamshire Hospital, Glossop Road, Sheffield S10 2JF, UK 35 Respiratory physiology and anaesthesia increases tidal volume, inspiratory flow and frequency. This is abruptly followed by a fall in ventilatory drive, accompanied by a fall in tidal volume, inspiratory flow and, possibly, a period of apnoea followed by more rapid shallow breaths. Propofol appears to abolish the response to hypoxaemia and is a potent depressor of chemoreceptor activity and upper airway reflexes. Ketamine is unusual; it is less depressant and associated with greater inspiratory flows and marked expiratory braking. Opioids have a powerful effect on respiratory drive. They prolong the expiratory pause, thus slowing respiratory rate and obtunding the response to rising PaCO2. They also suppress REM sleep and, therefore, increase rebound REM that occurs when they are discontinued. Benzodiazepines in premedicant doses usually decrease chemosensitivity. Airway obstruction is a major risk, especially in elderly patients whose level of arousal has been reduced by regional anaesthesia. α2Adrenergic agonists can produce sedation and have been shown to decrease the response to elevations in PaCO2, so reducing the gradient of the ventilation response CO2 curve, but not the resting response. Intravenous lidocaine (1.5 mg kg–1) slows respiratory rate by increasing expiratory time and reduces tidal volume. Doxapram is a central ventilatory stimulant that leads to increased respiratory drive, increasing tidal volume and, to a lesser extent, respiratory rate. Chemoreceptors Peripheral and central chemoreceptors provide inputs to the respiratory centres. The peripheral chemoreceptors lie in the carotid and aortic bodies. The carotid bodies are more important in stimulating ventilation, while the aortic bodies are also capable of responding to hypotension. The peripheral chemoreceptors in both sites respond to hypoxaemia (unlike the central receptors), hypercapnia and hydrogen ion concentration. The carotid body receives a very high blood flow, enabling it to respond rapidly to changes in partial pressure. The bodies consist of structural type II cells and chemoreceptor type I or glomus cells, which contain many neurotransmitters. They appear to be inhibited by exogenous dopamine and α2-adrenergic agonists, but are stimulated by nicotine, atropine, doxapram and almitrine. The central chemoreceptors lie close to the origins of the glossopharyngeal and vagus nerves on the anterolateral surface of the medulla. They are within the blood brain barrier and are bathed in CSF. This slows the response of the central chemoreceptors relative to the peripheral sites. Carbon dioxide diffuses across the blood-brain barrier into the CSF, which 36 is less buffered than the plasma. This causes a fall in CSF pH which stimulates the central chemoreceptors. If PaCO2 is maintained at abnormal values for several days, CSF pH is restored to normal by changes in CSF bicarbonate. Sleep affects the changes which would normally be produced by the action of the chemoreceptors on the medulla, allowing PaCO2 to rise by 0.15–0.3 kPa in non-REM sleep and increasing the apnoeic threshold. The response to mechanical loading on the inspiratory system is reduced in non-REM sleep. These effects are greater in REM sleep but more difficult to assess because of irregular breathing patterns associated with this stage of sleep. REM sleep also results in increased airway resistance and decreased upper airway tone, potentially increasing the risk of upper airway obstruction. Ventilation – PaO2 response curve The relationship is a rectangular hyperbola, with little response to high values of PaO2. Ventilation begins to increase at a PaO2 of 7–8 kPa and rapidly at 4.3 kPa. Sudden acute hypoxaemia stimulates ventilation within a few seconds. Ventilation – PaCO2 response curve The response is slower than that of hypoxaemia but is linear up to high values of PaCO2. However, ventilation becomes depressed at values of somewhere between 13 and 26 kPa. The response curves have the same gradient but are displaced to the left in acidosis. Opioids and inhalational agents displace the curve to the right and flatten the gradient. The gradient of the response curve for a given pH is steeper in hypoxaemia. The effect of anaesthesia on the upper airway Upper airway patency relies on the muscles of the upper airway. These are either dilators, which maintain patency, or constrictors, which are involved with swallowing. They are orientated in a radial direction to open the airway, e.g. levator veli palatini, or longitudinally acting on the hyoid bone to pull the airway open, e.g. geniohyoid and thyrohyoid (Fig. 1). When conscious, the airway will remain patent even in the presence of negative intrathoracic pressures of –60 cm H2O. However, when asleep, this falls to –13 cm H2O. Anaesthesia lowers the tone of the upper airway muscles and further promotes airway occlusion. Topical local anaesthesia of the upper airway increases airway resistance and makes collapse more likely. Agents such as benzodiazepines, barbiturates, alcohol and halothane reduce the activity of the nerves supplying the British Journal of Anaesthesia | CEPD Reviews | Volume 1 Number 2 2001 Respiratory physiology and anaesthesia Mandible Myelohyoid Geniohyoid Hyoid Hyoid displaced anteriorly Thyrohyoid Thyroid Fig. 1 Geniohyoid and thyrohyoid tense longitudinally, producing a force vector that displaces the hyoid anteriorly, assisting the maintenance of a patent upper airway (based on Drummond, 1996). upper airway more than they affect the diaphragm. However, ketamine maintains airway patency by promoting muscle activity. The sensitivity of different muscle groups to the effect of neuromuscular blockade varies. Importantly, the ability to cough or swallow and co-ordinate the larynx and upper airway may lag behind the recovery of the diaphragm. Narrowing of the airway with an ET tube or mucosal swelling results in increased resistance during inspiration and thus down-stream pressure becomes even more negative, further promoting airway collapse. Reflex responses occur in all parts of the upper airway, particularly in children, where laryngospasm and apnoeic responses to stimulation are common and a deep plane of anaesthesia is required if coughing, laryngospasm or bronchospasm are not to occur on stimulation. Propofol is particularly effective in overcoming upper airway reflexes. Coughing may occur on recovery at a depth of anaesthesia where regular respirations have not yet returned. The respiratory muscles Respiratory muscles can be subdivided into inspiratory and expiratory. Inspiratory muscles include the diaphragm, upper intercostals and parasternals and the accessory muscles (sternocleidomastoids, strap muscles of the neck, trapezius and the pectoral muscles when the shoulders are braced). Expiration is normally passive, but can be active using the lower intercostals and the abdominal muscles. Coughing additionally requires co-ordinated closing and opening of the glottis. The diaphragm is a bi-domed structure attached by the crura to the lumbar vertebrae. When this area contracts, it moves downward, producing a fall in intrathoracic pressure. The descent increases intra-abdominal pressure which is transmitted laterally to the lower rib cage via the zone of apposition where the diaphragm is flat against the adjacent pleura and the lower ribs. This forces the rib cage outward and, as the abdominal pressure rises, the abdominal contents act like a fulcrum which prevents further diaphragmatic descent as the diaphragm shortens. Therefore, the lateral margins of the diaphragm are pulled upward, further elevating and swinging the ribs into a more horizontal position. This widens and elevates the rib cage. Simultaneously, the intercostals and scalene muscles contract in a complex and rapid descending sequence, expanding, elevating and stabilising the rib cage. This lowers further intrapleural pressure and prevents the increasingly negative intrathoracic pressure from pulling the rib cage inwards. The intercostals and the abdominal muscles also aid in the maintenance of posture, while the external oblique and transverus abdominis are tonically active, keeping the diaphragm at the optimal stretch and shape. The effect of anaesthesia on the respiratory muscles General anaesthesia may affect the tone or strength of the respiratory muscles. This may explain why functional residual capacity (FRC) falls during the first 15–40 s after induction of anaesthesia. There is debate as to the relative contribution of the rib cage and the diaphragm and whether some of the changes are due to relaxation of postural muscles altering the position of the chest. FRC is reduced during anaesthesia employing a spontaneous breathing technique or positive pressure ventilation with paralysis. The fall in FRC, when measured using gas dilution techniques, may be exaggerated by gas trapping. However, other studies using specially adapted body box plethysmography, impedance plethysmography and spiral CT, have shown that this is not the only factor. Posture affects FRC, even in awake subjects. Using the example of a 70 kg male with an FRC of approximately 3 l, moving from the upright to supine position decreases FRC by 700 ml. Anaesthesia decreases FRC by another 300–500 ml, but some of this may be accounted for by further changes in body position as postural muscles relax. To eliminate this factor, measurements have been made while supporting the spine with a VacPac mattress to reduce skeletal movements. This British Journal of Anaesthesia | CEPD Reviews | Volume 1 Number 2 2001 37 Respiratory physiology and anaesthesia Excursion of diaphragm (anaesthetised, mechanical ventilation and neuromuscular blockade) Abdominal wall Rib cage Resting position of diaphragm Decreased functional residual capacity Blood volume Excursion of diaphragm (awake) Excursion of diaphragm (anaesthetised, spontaneous breathing) Fig. 2 The diaphragm (D) excursion when awake is compared with the anaesthetised state with spontaneous breathing and anaesthesia with paralysis and mechanical ventilation.The diaphragm is displaced rostrally during anaesthesia, but the excursion is primarily anteriorly during IPPV with paralysis and posteriorly during spontaneous breathing.The rib cage (RC) moves inwards, reducing FRC, as does the abdominal wall (AB).The central blood volume pools in the abdomen during mechanical ventilation. has demonstrated a fall in rib cage volume of approximately 300 ml after induction of anaesthesia with propofol, but no change in the abdominal compartment volume, suggesting that the position and shape of the diaphragm is less affected than those of the rib cage. There is evidence that tonic activity in the scalenes, sternocleidomastoids and, to a lesser extent, the intercostals, is abolished by thiopentone. The evidence for changes in position of the diaphragm is less clear. However, in the paralysed ventilated patient and during anaesthesia with spontaneous breathing, there is a significant cephalad displacement of the dome of the diaphragm. Therefore, changes in lung volume are likely to be due to a fall in chest wall tone with or without a fall in diaphragmatic tone (Fig. 2). The contribution of changes in disposition of the blood volume during spontaneous breathing to changes in FRC is not well established. It is possible that increasing intrathoracic blood volume could displace some of the air filled lung volume in the thorax. However, studies using inductive plethysmography, which measures change in total chest or abdominal volume regardless of the cause, suggest that, during quiet and unobstructed spontaneous breathing under anaesthesia, movement of blood into the thorax is not a major factor affecting FRC. More recent studies, using chest and abdominal CT 38 combined with central blood volume measurement by dye dilution and multiple breath nitrogen washout techniques, have suggested that blood pools in the abdomen during IPPV with paralysis and there is a reduction in the transverse area of the chest with cephalad movement of the diaphragm. Consequences of a fall in lung volume during anaesthesia Atelectasis occurs by three methods: (i) absorption of gases behind blocked airways; (ii) compression; and (iii) loss of surfactant. Fall in FRC has consequences for ventilation and perfusion. A decrease in lung volume will reduce traction on air passages and lead to a narrowing of bronchi and bronchioles leading to increased airway resistance, airway collapse and atelectasis. This results in reduced compliance and increased work of breathing. Compression atelectasis would occur particularly at the lung bases if there was a reduction in diaphragmatic tone allowing the pressure in the posterior upper abdomen to be transmitted to the lower posterior lung units. Indeed, rapid onset of postero-basal atelectasis has been visualised by CT, shortly after induction of anaesthesia. Closing volume (CV) is the lung volume at which small airway collapse begins. CV is >FRC in neonates and the over 40-year-olds. Anaesthesia reduces FRC close to, or below, closing volume in those in the middle age range. The effect is increased at the extremes of age, obesity and even in those with an abnormally high FRC, but poor lung elasticity and high resistance, e.g. emphysema. This causes airway closure and alveolar collapse. The lack of regular lung expansion will reduce the formation and spread of surfactant thus worsening the situation. Once airways close off, atelectasis will be hastened during periods of 100% oxygen administration or by the replacement of nitrogen with nitrous oxide. Ventilation-perfusion mismatch in anaesthesia Changes in lung volume and airway patency cause a mismatch of lung ventilation and perfusion (V/Q mismatch). The V/Q ratio may be very low or zero in areas that are perfused but not ventilated, or extremely high in those areas where there is ventilation but no perfusion (dead space). A range of states between these two extremes may exist, usually with good matching in most of the lung. During anaesthesia, these two extremes are more prevalent than in awake subjects. This has been confirmed by the finding of an increased spread of V/Q ratios during anaesthesia. British Journal of Anaesthesia | CEPD Reviews | Volume 1 Number 2 2001 Respiratory physiology and anaesthesia Hypoxic pulmonary vasoconstriction (HPV) normally reduces blood flow in areas of atelectasis, so promoting the matching of ventilation and perfusion. However, volatile agents impair this process, as alveolar anaesthetic concentration rises. For example, in human studies, HPV was reduced by 50% by 1 MAC halothane and 20% by isoflurane. Studies attempting to reduce atelectasis during anaesthesia have required airway pressures to be increased to 40 cm H2O for 15 s to re-open the airways. These pressures are above those normally seen during IPPV in theatre. Studies employing single photon emission computerised tomography to record the passage of radiolabelled aerosols and lung perfusion by radiolabelled albumin have shown that shunt is solely located in the atelectatic regions during anaesthesia. Reduction in FRC and amount of atelectasis is similar during anaesthesia with either spontaneous breathing or artificial ventilation. However, the lower-most dependent part of the diaphragm moves more during spontaneous breathing, suggesting that regional ventilation is different. During artificial ventilation, more gas passes to the upper (anterior) alveoli, which may become relatively overstretched, while the lower (posterior) alveoli are compressed by the weight of the heart and abdominal contents. Despite this, ventilation-perfusion studies have failed to find any great differences between the two types of anaesthesia, with shunt fractions of 1% awake, 11% during spontaneous breathing and 14% during artificial ventilation. Ketamine is once again unusual; during spontaneous breathing, no V/Q mismatch is seen. However, when artificial ventilation is commenced, areas of atelectasis and shunt begin to appear. breathing. This may be exacerbated by poor pain relief and increased ventilatory demands in the cold, shivering and catabolic postoperative patient. In this situation, the load on the respiratory system may exceed capacity and failure will occur. Adequate analgesia, routine use of warming techniques, intraoperative PEEP, ventilation regimes including air, extubation in a sitting up posture (where possible) and early use of postoperative CPAP may reduce these problems. Postoperative lung function Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ 2000; 321: 1493–7 Postoperative lung function is most impaired in patients with upper abdominal surgery because of basal atelectasis, V/Q mismatch, upper airway obstruction and increased work of Effect of regional anaesthesia on physiology, morbidity and mortality The effects depend on the extent of the blockade. Blocks which affect all lumbar and thoracic segments decrease inspiratory capacity by 20% and reduce expiratory reserve to almost zero. Expiratory muscle strength is greatly reduced during the action of lumbar spinal anaesthesia, temporarily reducing cough efficiency. However, most blocks are not so extensive and, in these situations, V/Q mismatch is close to the normal situation. Overall mortality is reduced by one-third in patients undergoing local anaesthesia. This is due, at least in part, to the significant reduction in respiratory complications including pulmonary emboli, respiratory depression and pneumonia especially after general, orthopaedic, urological and vascular surgery. Key references Drummond GB. Mechanics of breathing: effects of anaesthesia. In: PrysRoberts C, Brown B. (eds) International Practice of Anaesthesia: Oxford: Butterworth Heineman 1996; 1/59/1–26 Hedenstierna G, Rothen HU. Pulmonary gas exchange, effect of anaesthesia and of mechanical ventilation. In: Prys-Roberts C, Brown B. (eds) International Practice of Anaesthesia: Oxford: Butterworth Heineman 1996; 1/60/1–13 See multiple choice questions 17–21. British Journal of Anaesthesia | CEPD Reviews | Volume 1 Number 2 2001 39