Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
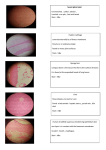
Infection disease I2 洪俊斌 CASE11 A 32-year-old woman with pain in her right eye was seen by her ophthalmologist, who diagnosed a corneal ulcer in the affected eye. Her physical examination was unremarkable otherwise; she had no history of eye problems and had recently been examined by her primarycare physician, who declared her to be in good health. Bacterial cultures taken from a discharge from her eye were negative. Viral cultures were also negative. Specimens were collected for culture for free-living amebae. No amebic parasite was recovered in culture. Figure 11.1 shows the parasite in a smear stained by the chromotrope Gram stain method. The Warthin-Starry silver stain was used to confirm the diagnosis. Picture Chromotrope Gram stain method In this method, the samples are stained in heated (50 degrees C to 55 degrees C) solutions of crystal violet and iodine used in Gram's stain, followed by a modified chromotrope solution (heated to 50 degrees C to 55 degrees C). The modified stain is composed of chromotrope 2R (1%), fast green (0.15%), and phosphotungstic acid (0.25%). Gram-chromotrope" staining technique can be used to detect microsporidian spores in clinical specimens(stool). How to think Right eye corneal ulcer Immunocompetent patient Chromotrope Gram stain(+) The Warthin-Starry silver stain(+) In microscopic view: Many spores like materials was seen in this specien: blue or black Microsporidian spores was highly suspected QUESTIONS Which group of obligate intracellular protozoan parasites fits the description given and might be causing this infection in this immunocompetent woman? ANS Microsporidia are obligately intracellular, spore-forming parasites belonging to the phylum Microspora and the order Microsporida. They are eukaryotic organisms containing 70S ribosomes but lacking mitochondria, peroxisomes, Golgi membranes, and other typically eukaryotic organelles. The phylum Microspora contains over 1000 species. The host range is extensive and includes honeybees, fish, mosquitoes, fleas, grasshoppers, rodents, rabbits, and other fur-bearing mammals. QUESTIONS List several members of this group that may be causing this patient's infection ANS seven genera Nosema corneae Vittaforma ocularum Enterocytozoon Encephalitozoon Pleistophora Trachipleistophora Brachiola QUESTIONS Which laboratory procedure may be used to identify the parasite to genus level? ANS Polymerase chain reaction is available in some research laboratories and can be used to diagnose the following 3 Encephalitozoon species: (1) E bieneusi, (2) V corneae, and (3) Nosema species QUESTIONS What are the structures seen in the smear? ANS The spore wall should stain pinkish to red, with the interior of the spore being clear or perhaps showing a horizontal or diagonal stripe, which represents the polar tube. The background will appear green or blue, depending on the method Arrow shows coiled polar filament. Silver stain Nosema connori QUESTIONS Which other laboratory procedures are available to diagnose infections with this group of protozoans? ANS Body fluid specimens – Microscopic examination of stained stool samples – Examine stools for other parasites (ova and parasite exam) and bacteria. – The modified trichrome stain (chromotrope 2R) commonly is used to detect microsporidia in urine, stool, or mucus. – The rapid Gram chromotrope method can be performed more quickly (about 11 min) and combines the chromotrope method with a Gram-staining step. The spores stain dark violet, and the equatorial stripe is enhanced. – Cytologic and histologic examinations are quite useful in diagnosis. A conjunctival scraping or swab frequently can reveal the organism after a Gram stain (organisms usually stain gram-positive) or chromotrope stain. – Stains that are used to detect microsporidia include the Brown Brenn Gram stain, WarthinStarry silver stain, Giemsa, and trichrome blue. – Fluorochrome stains, including calcofluor white and uvitex 2B, have a high affinity for chitin. – Microsporidia stain poorly with hematoxylineosin. Immunofluorescence assays using monoclonal or polyclonal antibodies are available in some research laboratories and can be performed on most specimens, QUESTIONS Describe the pathogenesis of this infection Humans acquire infection through ingestion or inhalation of spores. Studies isolating Encephalitozoon species in the urinary tract in those with disseminated infections suggest that sexual transmission is possible. The spore is the infective form. It is environmentally resistant and can survive for several months. The spore extrudes its polar tubule and injects the infective sporoplasm into the host cell. Once inside the cell, it multiplies by binary fission or schizogony. Development can occur directly inside the host cell cytoplasm or inside parasitophorous vacuoles. As mature spores develop and accumulate, the cell expands and eventually ruptures, releasing the spores. QUESTIONS How does this infection differ in immunocompromised (AIDS) patients? ANS – Immunocompetent patients with ocular involvement due to Encephalitozoon species can have conjunctival hyperemia. A slit lamp examination can reveal keratoconjunctivitis, which is characterized by diffuse, superficial, punctate keratopathy. Infection frequently is bilateral. – Corneal ulceration is rare in patients with AIDS. Retinal involvement is not reported. But chronic diarrhea and wasting can be found in some immunocompromised patients. – The symptom of corneal ulcer in immunocompromised patients is mild and the destruction of corneal is less serious than immunocompetent pateints due the low response of immunity,so the ocular symptoms are always neglected in some HIV infected patients. Thanks for your attention !!