Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
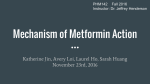
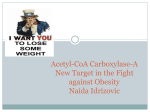
Advances in Arrhythmia and Electrophysiology AMP-Activated Protein Kinase Potential Role in Cardiac Electrophysiology and Arrhythmias Masahide Harada, MD, PhD*; Sarah Naomi Nattel, BA*; Stanley Nattel, MD Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 A AMPK phosphorylates a wide range of signaling systems and effectors, with major functional consequences (Figure 2). AMPK is a heterotrimeric enzyme with 1 catalytic (α) and 2 regulatory (β and γ) subunits (Figure 1). Thr-172 in the α-subunit is a crucial phosphorylation site that regulates AMPK function. The β-subunit has 2 structural components: a glycogen-binding domain that is sensitive to fuel storage levels and a C-terminal region that anchors α- and γ-subunits. The γ-subunit has a pair of cystathionine-β-synthase sequence repeats, called Bateman domains, which bind adenosine nucleotides.1–5 AMP binding to the γ-subunit facilitates Thr172 phosphorylation by upstream kinases, protects the site against dephosphorylation by protein phosphatases (PPs), and allosterically activates the enzyme. The crystal structure of AMPK has recently been resolved, revealing how the regulatory domain stabilizes the activation loop of the kinase domain and prevents dephosphorylation.6 Various isoforms of the AMPK subunits have been identified (α1, α2, β1, β2, γ1, γ2, γ3), potentially leading to the formation of 12 different complexes.1–5 The α2, β2, and γ2 subunits predominate in the heart, which mainly expresses α2/β2/γ2 complexes.1 Activated AMPK activation is favored by 3 nonexclusive mechanisms that often occur simultaneously: (1) allosteric activation, (2) α-subunit phosphorylation by upstream AMPK kinases (AMPKKs), and (3) inhibition of PP-mediated α-subunit dephosphorylation.1–6 AMP binding promotes AMPK activation by allosterically activating the enzyme, making it a poorer substrate for PPs and a better substrate for AMPKK.7 ADP binding also protects AMPK from dephosphorylation.6 Although the AMPK-binding affinity to ATP is high, its affinity for Mg-ATP, the predominant intracellular form, is much lower, explaining why ADP and AMP (with substantially lower physiological concentrations than ATP) can compete with ATP for binding.6 Metabolic dysfunction increases intracellular AMP concentrations, enhancing AMP binding to the cystathionine-β-synthase motifs in the γ-subunit. AMPK activation occurs with a half-maximally activating AMP concentration (A0.5) of 4 μmol/L and full activation by 10 μmol/L, within the physiologically attainable range.7,8 ATP antagonizes activation via AMP by competing with AMP for binding at the allosteric site, without promoting the active conformation.3 The A0.5 increases ≈20-fold when intracellular ATP concentration increases from 0.2 to 4 mmol/L.1 Phosphorylation of the α-subunit Thr-172 by upstream AMPKKs crucially regulates AMPK function. Combined AMPK activation by AMP and AMPK phosphorylation produces a >1000-fold increase in AMPK activity, whereas AMP alone elicits only a 5-fold maximum increase.3 Two major AMPKKs are present in the heart: liver kinase B1 (LKB1), also known as serine/threonine kinase 11,9 and Ca2+/calmodulin-dependent protein kinase kinase (CaMKK). LKB1 is much more abundantly expressed in the heart than CaMKK.2 The amphipathic αG-helix in the AMPK α-subunit interacts with LKB1.10 LKB1 reacts to myocardial ischemia by phosphorylating the α2-subunit.1 CaMKK, particularly the CaMKKβ (CaMKK2) isoform, phosphorylates and activates AMPK on elevation of intracellular Ca2+ concentration.4 MP-activated protein kinase (AMPK), a serine/threonine kinase, is a highly conserved homeostatic regulatory enzyme with a plethora of important roles in energy storage and use. ATP is the primary cellular energy source; in situations of metabolic deficiency, its breakdown product AMP accumulates. AMPK is sensitive to the cellular energy state: it is activated by AMP and inactivated by ATP. Under metabolic stress, when the AMP/ATP ratio is elevated, AMPK acts as an energy sensor and compensates for energy depletion by upregulating energy sources and downregulating energy-consuming processes that are not immediately essential.1–5 There is growing recognition that AMPK is particularly important in the heart, which demands more energy on a continuous basis than most other organs.1,2 AMPK seems to be a critical regulator of cardiac energy status and may be a potential therapeutic target. In this article, we will review the literature regarding cardiac AMPK and discuss evidence for a potentially important and underappreciated role of AMPK in cardiac electrophysiology and arrhythmia generation. Activation of AMPK AMPK Structure Received April 3, 2012; accepted May 30, 2012. From the Department of Medicine and Research Centre, Montreal Heart Institute and Université de Montréal, Montreal, Quebec, Canada (M.H., S.N.); Department of Biology, Stern College for Women, Yeshiva University, New York, NY (S.N.N.); Department of Pharmacology and Therapeutics, McGill University, Montreal, Quebec, Canada (S.N.). *These authors contributed equally to this article. Correspondence to Stanley Nattel, MD, Montreal Heart Institute Research Centre, 5000 Belanger St E, Montreal, Quebec, H1T 1C8, Canada. E-mail [email protected] (Circ Arrhythm Electrophysiol. 2012;5:860-867.) © 2012 American Heart Association, Inc. Circ Arrhythm Electrophysiol is available at http://circep.ahajournals.org 860 DOI: 10.1161/CIRCEP.112.972265 Harada et al AMPK and Cardiac Electrophysiology/Arrhythmias 861 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Figure 1. AMP-activated protein kinase (AMPK) activation. The AMPK complex consists of 3 different subunits: the α-subunit has a kinase domain (KD) that phosphorylates downstream targets, the β-subunit scaffolds the α and γ subunits, the γ-subunit binds AMP or ATP in a competitive manner. AMP binding to the γ-subunit causes a conformational change of the AMPK complex, which increases phosphorylation of the α-subunit at Thr-172, primarily by preventing dephosphorylation by protein phosphatases (PPs) and by promoting phosphorylation by AMPK-kinases (AMPKKs), such as liverkinase B1 (LKB1) and Ca2+/calmodulindependent protein kinase kinase (CaMKK). Thr-172 phosphorylation substantially increases AMPK enzyme activity. In addition, AMP itself allosterically enhances enzyme activity. The transforming growth factor-β–activated kinase, a member of the mitogen-activated protein kinase kinase family, is also implicated in AMPK activation.11 PPs, particularly PP2A and PP2C, regulate AMPK activity by dephosphorylating Thr-172. AMP binding to the γ-subunit induces a conformational change in the α-subunit that prevents AMPK dephosphorylation by PPs.3 AMPK and Cardiac Metabolism AMPK phosphorylates a variety of enzymes that play important roles in cardiac metabolism (Figure 2), with a net effect to increase energy availability. Fatty Acid Metabolism Once activated under conditions of metabolic stress, AMPK enhances cellular energy availability. AMPK stimulates fatty acid oxidation (a major cardiac energy source) by phosphorylating and inhibiting acetyl-CoA carboxylase, the rate-limiting enzyme in malonyl-CoA synthesis. Malonyl-CoA inhibits carnitine palmitoyltransferase-1, a mitochondrial enzyme that facilitates fatty acid entry into the mitochondria for oxidation. Phosphorylation of acetyl-CoA carboxylase by AMPK inactivates acetyl-CoA carboxylase, thereby inhibiting malonyl-CoA production.12 The resulting decrease in malonyl-CoA concentrations disinhibits Figure 2. Downstream targets and effects of activated AMP-activated protein kinase (AMPK). Arrows indicate proteins whose function is activated as a result of phosphorylation by AMPK; blunt ends designate inhibited proteins. The functions around the periphery correspond to the systems affected by AMPK regulation of the proteins shown. ACC indicates acetylCoA carboxylase; eEF2, eukaryotic elongation factor-2; eNOS, endothelial NO synthase; ERRα, estrogen-related receptor α; FABPpm, fatty acid binding protein; FAT/CD36, fatty acid transporter; GLUT4, glucose transporter 4; GP, glycogen phosphorylase; GS, glycogen synthase; HMGR, 3-hydroxy 3-methylglutaryl CoA reductase; mTOR, mammalian target of rapamycin; PCG-1α, transcriptional coactivator peroxisome proliferator-activated receptor-γ coactivator 1α; PFK2, phosphofructokinase-2;ULK-1, Unc51–like kinase; ROS, reactive oxygen species; NADPH, nicotinamide adenine dinucleotide phosphate. 862 Circ Arrhythm Electrophysiol August 2012 carnitine palmitoyltransferase-1 and promotes fatty acid oxidation.1,2,4,5,12 AMPK increases the expression of the fatty acid transporter fatty acid translocase/CD36 and membrane-associated fatty acid–binding protein, both of which are involved in cellular fatty acid uptake. AMPK also recruits lipoprotein lipase, which extracts fatty acid molecules from triglycerides and enhances fatty acid availability. Glucose Metabolism Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 AMPK is involved in carbohydrate metabolism, independently of insulin-mediated mechanisms. The AMPK-dependent regulation of carbohydrate metabolism is particularly important in pathological conditions, in which oxygen depletion and anaerobic glycolysis are of primary concern, whereas insulin-dependent regulation predominates at rest or during physiological stresses, such as exercise. Activated AMPK increases the protein expression of glucose transporters GLUT1 and GLUT4, increasing cellular glucose uptake. GLUT4 is also trafficked into the membrane from intracellular stores on AMPK activation.1 AMPK does not directly phosphorylate GLUT4: other AMPK targets, such as protein kinase C, p38 mitogen–activated protein kinase, and transforming growth factor-β–activated protein kinase 1–binding protein, may mediate the enhancement of GLUT4 function.13 Activated AMPK also phosphorylates phosphofructokinase-2 to convert fructose-6-phosphate to fructose-2,6-bisphosphate.1–5 Fructose-2,6-bisphosphate activates phosphofructokinase-1, which accelerates glycolysis. Therefore, AMPK activation promotes both glucose uptake and glycolysis. AMPK inhibits glycogen synthase (an enzyme that converts glucose to glycogen) and stimulates glycogen phosphorylase (an enzyme that results in the degradation of glycogen to glucose).1,2 5-Aminoimidazole-4-carboxamide1-β-D-ribofuranoside (a pharmacological AMPK activator) increases glycogen degradation in perfused rat hearts without altering glycogen synthase and glycogen phosphorylase activities.14 However, repeated AMPK activation increases glycogen content, and the precise roles of AMPK in the glycogen storage process are yet to be fully clarified.1 AMPK and Arrhythmia-Promoting Cardiovascular Disease A variety of important cardiac disease conditions alter cardiac ion channel and transporter function and promote arrhythmogenesis.15 Metabolic stress plays a central role in the cellular dysfunction caused by conditions such as hypertrophy, heart failure (HF), and myocardial ischemia (Figure 3). By alleviating cellular stress, AMPK plays an important adaptive role and can mitigate complications, presumably including arrhythmogenesis. Interestingly, although there is a strong body of evidence implicating AMPK as protective against arrhythmogenic disease conditions (see below), the actual information available about changes in arrhythmogenesis because of activation or inhibition of AMPK in such conditions is extremely limited. Cardiac Hypertrophy Cardiomyocyte hypertrophy is most apparent in response to pressure loads (eg, hypertension and valvular disease), although it occurs with any maintained increase in cardiac load. Cardiac hypertrophy increases metabolic demand, consuming more energy. Relative anoxia results from increased energy needs, as well as impaired coronary blood flow distribution because of altered diastolic transmural pressure gradients, inducing metabolic perturbations. Several studies have shown increased AMPK α-subunit phosphorylation in models of cardiac hypertrophy.16 Upregulated glucose and fatty acid metabolism with AMPK activation increases the availability of energy sources, which may mitigate metabolic stress. AMPK is also involved in downstream signaling processes regulating protein synthesis, such as mammalian target of rapamycin (mTOR), eukaryotic elongation factor-2 (eEF2), and p70S6 kinase (Figure 2).17 These signaling pathways increase protein synthesis and promote hypertrophic growth and proliferation. AMPK inhibits these cascades, countering cardiac hypertrophy.17 AMPK activation mitigates transverse aortic constriction–induced cardiac hypertrophy through inhibition of protein synthetic signaling.18,19 AMPK activation would thus be expected to combat the arrhythmogenic potential inherent in cardiac hypertrophic conditions,20 both by limiting metabolic disturbances caused by hypertrophy and by suppressing hypertrophy itself. Heart Failure AMPK prevents the progression from hypertrophy to HF: AMPK α2-subunit–deficient mice show exacerbated transverse aortic constriction–induced hypertrophy and accelerated transition to HF.21 Transition to HF is associated with activation of mTOR signaling, which is responsible for protein synthesis and cell proliferation. AMPK also stimulates autophagy via activation of Unc-51–like kinase that is suppressed by mTOR (Figure 2).22 Malfunction of mitochondrial biogenesis is an important component in the development of HF.23 Nuclear receptors and their coactivators, such as estrogen-related receptor α and peroxisome proliferator–activated receptor-γ coactivator 1α, regulate mitochondrial transcripts and stimulate fatty acid oxidation and oxidative respiration.24,25 Activation of AMPK increases expression levels of estrogen-related receptor α: AMPKα2 knockout mice have decreased estrogen-related receptor α expression, whereas constitutively active AMPK increases estrogen-related receptor α expression.24 AMPK activation also stimulates mitochondrial biogenesis via direct phosphorylation of peroxisome proliferator–activated receptor-γ coactivator 1α.25 Both these effects lead to improved mitochondrial function and could, therefore, protect against HF. Cardiac angiogenesis concomitant with hypertrophy is also critical for slowing the transition to HF. AMPK activation increases the expression of proangiogenic factors, such as endothelial NO synthase and vascular endothelial growth factor.11 Adiponectin has pleiotropic cardioprotective effects and activates AMPK. In adiponectin-deficient mice, impaired AMPK activation accelerates the transition to HF in transverse aortic constriction–induced hypertrophy because of inadequate angiogenesis.26 AMPK decreases endoplasmic stress in endothelial cells and prevents cellular apoptosis in cardiomyocytes.27 AMPK inhibits nicotinamide adenine dinucleotide phosphate-oxidase activation and thereby reduces reactive oxygen species Harada et al AMPK and Cardiac Electrophysiology/Arrhythmias 863 Figure 3. AMP-activated protein kinase (AMPK) in arrhythmia-promoting cardiovascular pathology. Cardiac disease–related processes (eg, hypertrophy, congestive heart failure [CHF], and ischemia/reperfusion) facilitate arrhythmia generation by causing cellular dysfunction and inducing metabolic stress. AMPK activation in response to metabolic stress improves metabolic disturbances and cellular dysfunction. FA indicates fatty acid. Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 generation.9 These effects might also contribute to preventing transition to HF. It must be pointed out that actions of AMPK are not necessarily beneficial in all cardiac failure paradigms. For example, a recent study suggests that AMPK activation may mediate ethanol-induced myocardial hypocontractility via enhanced AMPK-mTOR-Unc-51–like kinase–mediated autophagy.28 Myocardial Ischemia and Reperfusion Injury AMPK is particularly important during ischemia and ischemia/reperfusion injury. Oxidative metabolism decreases under ischemic conditions, and anaerobic glycolysis predominates. AMPK accelerates glucose metabolism in response to an increased AMP/ATP ratio. The metabolic state of the postischemic myocardium is a critical determinant of myocardial injury and recovery of cardiac function upon reperfusion. Using transgenic mice overexpressing nonfunctional (kinase dead) AMPK, Russell et al29 demonstrated that kinase-dead AMPK hearts fail to augment glucose and fatty acid metabolism during ischemia/reperfusion, manifesting increased myocardial injury. Substantial energy resources are consumed to incorporate amino acids into protein. AMPK activation limits energy consumption by suppressing protein synthetic signaling pathways, such as eEF-2 and mTOR.30 Although myocardial necrosis is primarily responsible for cell death during ischemia/reperfusion, apoptosis also contributes. The increased myocardial damage in kinase-dead AMPK hearts subjected to ischemia/reperfusion is also because of increased apoptosis.29 The antiapoptotic effect of adiponectin is also mediated by the activation of AMPK.31 AMPK and Cardiac Electrophysiology/Arrhythmias PRKAG2 Mutation Cardiomyopathy The most striking example of arrhythmogenesis related to AMPK dysfunction is protein kinase, AMP-activated, γ2 noncatalytic subunit (PRKAG2) mutation cardiomyopathy. Humans with missense mutations in the γ2 regulatory subunit of AMPK (PRKAG2) have hypertrophic cardiomyopathies and frequently manifest arrhythmogenic electrophysiological abnormalities.1,32,33 The pathology caused by the diseaseproducing PRKAG2 mutations Arg302Gln, Thr400Asn, and Asn488Ile is characterized by preexcitation, atrial fibrillation (AF), progressive conduction system disease, and cardiac hypertrophy.32,33 Mice overexpressing PRKAG2 genes with disease-causing mutations R302Q, N488I, or R531G in the heart recapitulate the phenotype of human PRKAG2 cardiomyopathy.34–36 The effects of these mutations on AMPK function is complex: they seem to enhance basal activity but impair activation because of AMP accumulation.1 Histological findings include an abundance of vacuoles and increased periodic acid-Schiff-positive materials, indicating increased glycogen deposition. Myofiber disarray, typical of hypertrophic cardiomyopathy, is not detected, and interstitial fibrosis is minimal, although the myocytes are enlarged. Ventricular preexcitation and supraventricular tachyarrhythmia are observed in most of the transgenic animals. Patel et al34 demonstrated that the annulus fibrosis, which limits electrical connection between the atria and ventricles, is thinned, stretched, and disrupted in N488I-expressing transgenic mice and that this region contains many vacuolated, glycogen-loaded myocytes. These data suggest that PRKAG2 cardiomyopathy and the associated preexcitation are attributable to a glycogen storage abnormality distinct from hypertrophic cardiomyopathy. Developmental abnormalities lead to failure of formation of a complete annulus fibrosis, preserving atrioventricular muscle bundle connections. The effect of N4881 PRKAG2 mutations is specific for AMPK containing α2-subunits; AMPK containing α1-subunits is unaffected.37 Ion Channel Regulation and Other Determinants of Arrhythmia Figure 4 shows the potential effects of AMPK on a variety of arrhythmia determinants, including ion channels, transporters, and structural factors. The open-state inactivation of cardiac voltage-gated Na+ channels is slowed in mice overexpressing a 864 Circ Arrhythm Electrophysiol August 2012 Figure 4. AMP-activated protein kinase (AMPK)–dependent modification of factors governing cardiac arrhythmogenesis. Activated AMPK can directly regulate ion channel/transporter function, altering cardiac electrophysiological function and thereby modifying cardiac arrhythmogenesis. In addition, effects on cell proliferation and hypertrophy can modify cardiac structure to alter arrhythmogenic substrates. Most of the effects shown are directly induced by AMPK; however, changes in SERCA and PLB have been observed in models of AMPK knockdown and may be secondary to a cardiomyopathic phenotype. NCX indicates Na+/Ca2+-exchanger; PLB, phospholamban; RyR2, ryanodine receptor type-2 (cardiac form); SERCA, sarcoplasmic reticulum Ca2+-ATPase; DADs, delayed afterdepolarizations. Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 constitutively active mutant (T172D) of the AMPK α1-subunit.38 This induces a gain in late Na+-channel function, increasing action potential duration (APD) and causing early afterdepolarizations, similar to long-QT syndromes caused by SCN5Aa mutations.38 Thus, basal AMPK activation due to PRKAG2 mutations may be arrhythmogenic by altering Na+-channel function. Delayed repolarization is a well-recognized consequence of HF that contributes to arrhythmogenesis15; one of the causes may be incomplete Na+-channel inactivation due to AMPK activation secondary to HF-induced metabolic stress. AMPK has potentially significant effects on cardiac K+ channels. Ischemic preconditioning involves myocardial ATPdependent K+ (KATP) channels. Mice expressing dominantnegative AMPK α2-subunits (functional AMPK-knockdown) lack preconditioning-induced activation of KATP channels, APD shortening, and cardioprotection.39 The authors provided evidence suggesting that AMPK may be needed to enhance trafficking of KATP channels to the sarcolemma on preconditioning. Phenylephrine-induced cardiac preconditioning also seems to require AMPK-related sarcolemmal KATP-channel activation.40 Although in the case of preconditioning AMPKrelated APD abbreviation may contribute to cardioprotection, the same effect could promote the risk of malignant reentrant arrhythmias during acute myocardial ischemia/infarction. An important recent study showed that AMPK binds directly to KATP channels and AMPK activation enhances KATP open probability during metabolic inhibition.41 This observation raises the possibility that low-micromolar AMP concentrations, as seen in early ischemia and possibly intense exercise, open KATP channels by activating AMPK. This action could be an important contributor to cardioprotection but could also contribute to arrhythmogenesis by reducing APD and promoting reentry. AMPK has been shown to affect a variety of cardiac-expressed ion channels in noncardiac systems. AMPK phosphorylation of specific sites on Kv2.1 channels causes hyperpolarizing voltage shifts in activation and inactivation gating of neuronal Kv2.1 channels.42 AMPK inhibits KCa3.1 (SK1) Ca2+-activated K+ channels in human embryonic kidney cells.43 The Kir2.1 subunit that underlies inward-rectifier IK1 background outward currents maintaining the cardiomyocyte resting potential is regulated by AMPK when expressed in Xenopus oocytes.44 AMPK reduces Kir2.1 membrane expression and current, apparently by phosphorylating the ubuiquitin ligase Nedd4-2.44 A similar type of regulation occurs for the potassium voltage-gated channel, KCNQ1 (KQT-like subfamily, member 1)/potassium voltagegated channel, KCNE1 (Isk-related family, member 1 channel) that underlies cardiac IKs. If cardiac IK1 and IKs channels are similarly controlled by AMPK in situ, AMPK activation might downregulate their expression, causing eventual APD prolongation as seen with myocardial ischemia or HF.15 In the case of ischemia, this might lead to a biphasic response as has been observed experimentally,15 with initial APD reduction due to KATP activation, followed by normalization and then APD prolongation due to IK1/IKs downregulation. Ca2+ is a central regulator of a wide range of cellular functions, including important cardiac electrophysiological determinants.46 Although relatively little is known about AMPK regulation of cardiac Ca2+ handling, there are suggestions that it might be significant. Turdi et al47 examined interactions between aging and AMPK in the control of Ca2+ handling and contractility in mice. AMPK kinase-dead young mice showed almost no functional abnormalities other than reduced contractility at rapid rates. Aging reduced AMPK function, expression of the sarcoplasmic reticulum Ca2+-uptake pump, sarcoplasmic reticulum Ca2+-ATPase-2A (SERCA2A) and contractility, while increasing reactive oxygen species levels and causing cardiomyocyte hypertrophy. Elderly kinase-dead mice demonstrated enhancement of the aging-dependent changes, as well as reduced systolic [Ca2+]-transients and downregulation of the sarcoplasmic reticulum Ca2+-ATPase-2A–inhibiting protein phospholamban. Treatment with an AMPK activator, metformin, attenuated physiological aging-induced cardiomyocyte contractile defects. Thus, AMPK contributes to the regulation Harada et al AMPK and Cardiac Electrophysiology/Arrhythmias 865 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 of Ca2+ handling and contractile function, and a decrease in AMPK function with aging reduces cardiac contractility. Ikeda et al48 developed cardiomyocyte-specific LKB1 knockout mice and demonstrated a crucial role of the LKB1/ AMPK axis in maintaining cardiac function. LKB1 knockout mice had attenuated AMPK α2-subunit activation, enhanced protein synthetic signaling (via mTOR and eEF-2), and cardiomyocyte hypertrophy. They also showed impaired contractility in association with decreased phospholamban and sarcoplasmic reticulum Ca2+-ATPase-2 mRNA/protein expression and had significant atrial dilation along with spontaneous AF. In addition to direct electrophysiological effects mediated by altered ion channel and transporter function, AMPK might affect arrhythmogenesis indirectly by altering cellular processes that impact indirectly on arrhythmia risk. For example, AMPK-induced reductions in cell proliferation could decrease the likelihood of cardiac tissue fibrosis, an important arrhythmia-promoting change.49 Similarly, antihypertrophic effects of AMPK could reduce the likelihood of reentrant arrhythmia by preventing increases in cardiac mass.50 Evidence for a Role in Arrhythmias Despite important AMPK regulation of many arrhythmia- controlling factors and conditions (Figure 4), data regarding the involvement of AMPK in arrhythmias per se are quite limited. The only 2 clear-cut demonstrations of arrhythmogenesis resulting from primary disturbances in AMPK function are the mouse models of PRKAG2 cardiomyopathy associated with inducible orthodromic AV-reentrant tachycardia36 and of LKB1 deletion with spontaneous AF.48 With LKB1 deletion, AF occurs in a context of substantial structural remodeling and is not necessarily directly attributable to AMPK dysfunction. Other observations suggest a role of AMPK in controlling arrhythmogenesis but are not definitive. Barth et al51,52 found a relationship between metabolic alterations and permanent AF in human cardiomyocytes; transcripts involved in carbohydrate metabolism were significantly upregulated in atrial tissues from AF patients, whereas transcripts involved in fatty acid metabolism were downregulated. Recent metabolomic and proteomic analyses in human AF also demonstrate significant changes in the atrial enzymes and metabolites responsible for glycolysis and fatty acid oxidation, consistent with metabolic stress.53 A lower ratio of glycolytic/lipid metabolism end products was associated with early onset of postoperative AF, suggesting that metabolic disturbances increase AF vulnerability. This notion is supported by experiments showing that the inhibition of glycolysis promotes the occurrence of spontaneous AF in Langendorff-perfused rat hearts.54 In an electrically maintained AF model in goats, phosphocreatine decreased by 60% in atrial myocytes within 1 week, suggesting increased energy demand and expenditure during the early phases of AF.55 It is well known that HF promotes atrial and ventricular arrhythmogenesis.15 Cha et al56 demonstrated that dogs with Figure 5. Metabolic stress–related mechanisms in atrial fibrillation (AF) and possible role of AMP-activated protein kinase (AMPK). Increased cellular workload during the rapid atrial activation in AF increases energy demand and expenditure. The consequent metabolic stress limits the availability of ATP that controls cellular integrity and channel/transporter protein function. AF-induced dysregulation of ion channels, such as ICa-L and INa, causes action potential duration (APD)/wavelength (WL) shortening and conduction velocity (CV) slowing, which stabilizes reentrant mechanisms maintaining AF. Abnormal Ca2+ handling causes hypocontractility and atrial dilation that contributes to the AF substrate, as well as triggered arrhythmia mechanisms. In addition, enhanced production of reactive oxygen species (ROS) because of metabolic stress damages cellular macromolecules to cause AF-promoting dysfunction. AF-induced metabolic stress reduces the ratios of AMP/ATP and ADP/ATP, activating AMPK. AMPK activation should increase energy production (fatty acid/glucose metabolism) and limits energy consumption (protein synthesis), thereby counteracting the AF-induced metabolic stress. AMPK might also regulate ion channel function via direct phosphorylation. Changes in black have been observed experimentally; those in gray have not yet been examined but would be expected to occur. RyR2 indicates ryanodine receptor type-2; NCX, Na+/Ca2+-exchanger; SERCA2, sarcoplasmic reticulum Ca2+-ATPase; PLB, phospholamban; Tn-I, troponin-I; MyBP-C, myosin binding protein C; mTOR, mammalian target of rapamycin. 866 Circ Arrhythm Electrophysiol August 2012 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 dilated cardiomyopathic phenotypes caused by ventricular tachypacing have important defects in atrial bioenergetics, with depletion of ATP and creatine kinase, and that the propensity for AF is inversely related to atrial cellular ATP concentration. Another study in the same model showed profound changes in the expression of metabolic proteins and metabolites, with increased ADP/ATP ratio and a shift from glycolysis to α-ketoacid metabolism after 2 weeks of ventricular tachypacing.57 The glycolytic system was upregulated at 24 hours of ventricular tachypacing, suggesting an early response to increase energy output in the face of increased demands, with longer-term energy-preserving adaptations.57 There is thus extensive evidence for a role of metabolic stress in AF. Figure 5 shows a schema illustrating the potential involvement of metabolic abnormalities and AMPK in AF. AF induces metabolic stress by virtue of an increased workload due to a much increased atrial rate. Biochemical derangements resulting from metabolic stress alter ion channel function in ways that promote arrhythmia induction and maintenance, creating a positive feedback circuit. AMPK activation would be expected, based on the observed increase in ADP/ATP ratio57 and a likely concomitant rise in the AMP/ATP ratio. AMPK-induced phosphorylation would be expected to increase energy availability and reduce demands. If so, modulation of the AMPK system might provide a useful therapeutic target, and failed or deficient AMPK activation could promote AF in some cases. AMPK may also be a mediator of antiarrhythmic drug properties. Resveratrol has important AMPK-activating properties19,58 and is antiarrhythmic.59 Although the compound may have direct ion channel effects, it is conceivable that AMPK activation contributes to its beneficial effects on arrhythmias.59 Conclusions Emerging evidence demonstrates a close relationship between metabolic disturbances and cardiac electrophysiology and suggests the ability of AMPK to regulate a wide range of determinants of electrophysiological function and arrhythmogenesis. However, relatively little work has been done to address directly the participation of AMPK in cardiac electrical function and arrhythmias. Much more research is required to complete our understanding of the susceptibility of cardiac ion channels and transporters to modulation by AMPK activation, as well as to understand the involvement of AMPK in controlling arrhythmogenesis in pathological states. AMPK activation may play a protective role in some contexts and a proarrhythmic role in others—clarification of its consequences in specific contexts will be important. Present antiarrhythmic drug therapy is limited by poor efficacy and significant adverse effect risk: improved mechanistic understanding of arrhythmias may hold the key to ameliorating therapeutic potential.60,61 A better appreciation of the role of this important enzyme in controlling electrical activity in the normal and diseased heart might lead to important new mechanistic insights and potentially to new therapeutic opportunities. Acknowledgment We thank France Thériault for expert secretarial assistance with the manuscript. Sources of Funding This work was funded by Canadian Institutes of Health Research (MGP 6957 and MOP 68929), European-North American Atrial Fibrillation Research Alliance (ENAFRA; 07CVD03) of Fondation Leducq, and Quebec Heart and Stroke Foundation. Disclosures None. References 1. Arad M, Seidman CE, Seidman JG. AMP-activated protein kinase in the heart: role during health and disease. Circ Res. 2007;100:474–488. 2. Dyck JR, Lopaschuk GD. AMPK alterations in cardiac physiology and pathology: enemy or ally? J Physiol (Lond). 2006;574(Pt 1):95–112. 3. Viollet B, Horman S, Leclerc J, Lantier L, Foretz M, Billaud M, Giri S, Andreelli F. AMPK inhibition in health and disease. Crit Rev Biochem Mol Biol. 2010;45:276–295. 4. Towler MC, Hardie DG. AMP-activated protein kinase in metabolic control and insulin signaling. Circ Res. 2007;100:328–341. 5.Hardie DG, Hawley SA, Scott JW. AMP-activated protein kinase– development of the energy sensor concept. J Physiol (Lond). 2006;574 (Pt 1):7–15. 6. Xiao B, Sanders MJ, Underwood E, Heath R, Mayer FV, Carmena D, Jing C, Walker PA, Eccleston JF, Haire LF, Saiu P, Howell SA, Aasland R, Martin SR, Carling D, Gamblin SJ. Structure of mammalian AMPK and its regulation by ADP. Nature. 2011;472:230–233. 7. Frederich M, Balschi JA. The relationship between AMP-activated protein kinase activity and AMP concentration in the isolated perfused rat heart. J Biol Chem. 2002;277:1928–1932. 8. Hardie DG, Salt IP, Hawley SA, Davies SP. AMP-activated protein kinase: an ultrasensitive system for monitoring cellular energy charge. Biochem J. 1999;338(Pt 3):717–722. 9. Sakamoto K, Zarrinpashneh E, Budas GR, Pouleur AC, Dutta A, Prescott AR, Vanoverschelde JL, Ashworth A, Jovanovic A, Alessi DR, Bertrand L. Deficiency of LKB1 in heart prevents ischemia-mediated activation of AMPKalpha2 but not AMPKalpha1. Am J Physiol Endocrinol Metab. 2006;290:E780–E788. 10. Scholz R, Suter M, Weimann T, Polge C, Konarev PV, Thali RF, Tuerk RD, Viollet B, Wallimann T, Schlattner U, Neumann D. Homo-oligomerization and activation of AMP-activated protein kinase are mediated by the kinase domain alphaG-helix. J Biol Chem. 2009;284:27425–27437. 11. Fisslthaler B, Fleming I. Activation and signaling by the AMP-activated protein kinase in endothelial cells. Circ Res. 2009;105:114–127. 12.Ruderman NB, Saha AK, Kraegen EW. Minireview: malonyl CoA, AMP-activated protein kinase, and adiposity. Endocrinology. 2003; 144:5166–5171. 13.Li J, Miller EJ, Ninomiya-Tsuji J, Russell RR 3rd, Young LH. AMPactivated protein kinase activates p38 mitogen-activated protein kinase by increasing recruitment of p38 MAPK to TAB1 in the ischemic heart. Circ Res. 2005;97:872–879. 14.Longnus SL, Wambolt RB, Parsons HL, Brownsey RW, Allard MF. 5-Aminoimidazole-4-carboxamide 1-beta-D-ribofuranoside (AICAR) stimulates myocardial glycogenolysis by allosteric mechanisms. Am J Physiol Regul Integr Comp Physiol. 2003;284:R936–R944. 15. Nattel S, Maguy A, Le Bouter S, Yeh YH. Arrhythmogenic ion-channel remodeling in the heart: heart failure, myocardial infarction, and atrial fibrillation. Physiol Rev. 2007;87:425–456. 16. Tian R, Musi N, D’Agostino J, Hirshman MF, Goodyear LJ. Increased adenosine monophosphate-activated protein kinase activity in rat hearts with pressure-overload hypertrophy. Circulation. 2001;104:1664–1669. 17. Beauloye C, Bertrand L, Horman S, Hue L. AMPK activation, a preventive therapeutic target in the transition from cardiac injury to heart failure. Cardiovasc Res. 2011;90:224–233. 18. Li HL, Yin R, Chen D, Liu D, Wang D, Yang Q, Dong YG. Long-term activation of adenosine monophosphate-activated protein kinase attenuates pressure-overload-induced cardiac hypertrophy. J Cell Biochem. 2007;100:1086–1099. 19. Chan AY, Dolinsky VW, Soltys CL, Viollet B, Baksh S, Light PE, Dyck JR. Resveratrol inhibits cardiac hypertrophy via AMP-activated protein kinase and Akt. J Biol Chem. 2008;283:24194–24201. 20. Furukawa T, Kurokawa J. Potassium channel remodeling in cardiac hypertrophy. J Mol Cell Cardiol. 2006;41:753–761. Harada et al AMPK and Cardiac Electrophysiology/Arrhythmias 867 Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 21. Zhang P, Hu X, Xu X, Fassett J, Zhu G, Viollet B, Xu W, Wiczer B, Bernlohr DA, Bache RJ, Chen Y. AMP activated protein kinase-alpha2 deficiency exacerbates pressure-overload-induced left ventricular hypertrophy and dysfunction in mice. Hypertension. 2008;52:918–924. 22. Lee JW, Park S, Takahashi Y, Wang HG. The association of AMPK with ULK1 regulates autophagy. PLoS One. 2010;5:e15394. 23. Karamanlidis G, Nascimben L, Couper GS, Shekar PS, del Monte F, Tian R. Defective DNA replication impairs mitochondrial biogenesis in human failing hearts. Circ Res. 2010;106:1541–1548. 24. Hu X, Xu X, Lu Z, Zhang P, Fassett J, Zhang Y, Xin Y, Hall JL, Viollet B, Bache RJ, Huang Y, Chen Y. AMP activated protein kinase-a2 regulates expression of estrogen-related receptor-a, a metabolic transcription factor related to heart failure development. Hypertension. 2011;58:696–703. 25. Ventura-Clapier R, Garnier A, Veksler V. Transcriptional control of mitochondrial biogenesis: the central role of PGC-1alpha. Cardiovasc Res. 2008;79:208–217. 26. Shimano M, Ouchi N, Shibata R, Ohashi K, Pimentel DR, Murohara T, Walsh K. Adiponectin deficiency exacerbates cardiac dysfunction following pressure overload through disruption of an AMPK-dependent angiogenic response. J Mol Cell Cardiol. 2010;49:210–220. 27. Dong Y, Zhang M, Liang B, Xie Z, Zhao Z, Asfa S, Choi HC, Zou MH. Reduction of AMP-activated protein kinase alpha2 increases endoplasmic reticulum stress and atherosclerosis in vivo. Circulation. 2010;121:792–803. 28. Guo R, Ren J. Deficiency in AMPK attenuates ethanol-induced cardiac contractile dysfunction through inhibition of autophagosome formation. Cardiovasc Res. 2012;94:480–91. 29. Russell RR 3rd, Li J, Coven DL, Pypaert M, Zechner C, Palmeri M, Giordano FJ, Mu J, Birnbaum MJ, Young LH. AMP-activated protein kinase mediates ischemic glucose uptake and prevents postischemic cardiac dysfunction, apoptosis, and injury. J Clin Invest. 2004;114:495–503. 30. Young LH. AMP-activated protein kinase conducts the ischemic stress response orchestra. Circulation. 2008;117:832–840. 31. Shibata R, Sato K, Pimentel DR, Takemura Y, Kihara S, Ohashi K, Funahashi T, Ouchi N, Walsh K. Adiponectin protects against myocardial ischemia-reperfusion injury through AMPK- and COX-2-dependent mechanisms. Nat Med. 2005;11:1096–1103. 32. Gollob MH, Green MS, Tang AS, Gollob T, Karibe A, Ali Hassan AS, Ahmad F, Lozado R, Shah G, Fananapazir L, Bachinski LL, Roberts R, Hassan AS. Identification of a gene responsible for familial Wolff-Parkinson-White syndrome. N Engl J Med. 2001;344:1823–1831. 33. Sternick EB, Oliva A, Gerken LM, Magalhães L, Scarpelli R, Correia FS, Rego S, Santana O, Brugada R, Wellens HJ. Clinical, electrocardiographic, and electrophysiologic characteristics of patients with a fasciculoventricular pathway: the role of PRKAG2 mutation. Heart Rhythm. 2011;8:58–64. 34. Patel VV, Arad M, Moskowitz IP, Maguire CT, Branco D, Seidman JG, Seidman CE, Berul CI. Electrophysiologic characterization and postnatal development of ventricular pre-excitation in a mouse model of cardiac hypertrophy and Wolff-Parkinson-White syndrome. J Am Coll Cardiol. 2003;42:942–951. 35.Davies JK, Wells DJ, Liu K, Whitrow HR, Daniel TD, Grignani R, Lygate CA, Schneider JE, Noël G, Watkins H, Carling D. Characterization of the role of gamma2 R531G mutation in AMP-activated protein kinase in cardiac hypertrophy and Wolff-Parkinson-White syndrome. Am J Physiol Heart Circ Physiol. 2006;290:H1942–H1951. 36. Sidhu JS, Rajawat YS, Rami TG, Gollob MH, Wang Z, Yuan R, Marian AJ, DeMayo FJ, Weilbacher D, Taffet GE, Davies JK, Carling D, Khoury DS, Roberts R. Transgenic mouse model of ventricular preexcitation and atrioventricular reentrant tachycardia induced by an AMP-activated protein kinase loss-of-function mutation responsible for Wolff-ParkinsonWhite syndrome. Circulation. 2005;111:21–29. 37.Ahmad F, Arad M, Musi N, He H, Wolf C, Branco D, Perez-Atayde AR, Stapleton D, Bali D, Xing Y, Tian R, Goodyear LJ, Berul CI, Ingwall JS, Seidman CE, Seidman JG. Increased alpha2 subunitassociated AMPK activity and PRKAG2 cardiomyopathy. Circulation. 2005;112:3140–3148. 38. Light PE, Wallace CH, Dyck JR. Constitutively active adenosine monophosphate-activated protein kinase regulates voltage-gated sodium channels in ventricular myocytes. Circulation. 2003;107:1962–1965. 39. Sukhodub A, Jovanovic S, Du Q, Budas G, Clelland AK, Shen M, Sakamoto K, Tian R, Jovanovic A. AMP-activated protein kinase mediates preconditioning in cardiomyocytes by regulating activity and trafficking of sarcolemmal ATP-sensitive K(+) channels. J Cell Physiol. 2007;210:224–236. 40. Turrell HE, Rodrigo GC, Norman RI, Dickens M, Standen NB. Phenylephrine preconditioning involves modulation of cardiac sarcolemmal K(ATP) current by PKC delta, AMPK and p38 MAPK. J Mol Cell Cardiol. 2011;51:370–380. 41.Yoshida H, Bao L, Kefaloyianni E, Taskin E, Okorie U, Hong M, Dhar-Chowdhury P, Kaneko M, Coetzee WA. AMP-activated protein kinase connects cellular energy metabolism to KATP channel function. J Mol Cell Cardiol. 2012;52:410–418. 42. Ikematsu N, Dallas ML, Ross FA, Lewis RW, Rafferty JN, David JA, Suman R, Peers C, Hardie DG, Evans AM. Phosphorylation of the voltagegated potassium channel Kv2.1 by AMP-activated protein kinase regulates membrane excitability. Proc Natl Acad Sci U S A. 2011;108:18132–18137. 43. Klein H, Garneau L, Trinh NT, Privé A, Dionne F, Goupil E, Thuringer D, Parent L, Brochiero E, Sauvé R. Inhibition of the KCa3.1 channels by AMP-activated protein kinase in human airway epithelial cells. Am J Physiol Cell Physiol. 2009;296:C285–C295. 44. Alesutan I, Munoz C, Sopjani M, Dërmaku-Sopjani M, Michael D, Fraser S, Kemp BE, Seebohm G, Föller M, Lang F. Inhibition of Kir2.1 (KCNJ2) by the AMP-activated protein kinase. Biochem Biophys Res Commun. 2011;408:505–510. 45. Alesutan I, Föller M, Sopjani M, Dërmaku-Sopjani M, Zelenak C, Fröhlich H, Velic A, Fraser S, Kemp BE, Seebohm G, Völkl H, Lang F. Inhibition of the heterotetrameric K+ channel KCNQ1/KCNE1 by the AMP-activated protein kinase. Mol Membr Biol. 2011;28:79–89. 46. Nattel S, Dobrev D. The multidimensional role of calcium in atrial fibrillation pathophysiology: mechanistic insights and therapeutic opportunities. Eur Heart J. Available at http://www.ncbi.nlm.nih.gov/pubmed/22507975. Accessed on April 16, 2012. 47.Turdi S, Fan X, Li J, Zhao J, Huff AF, Du M, Ren J. AMP-activated protein kinase deficiency exacerbates aging-induced myocardial contractile dysfunction. Aging Cell. 2010;9:592–606. 48. Ikeda Y, Sato K, Pimentel DR, Sam F, Shaw RJ, Dyck JR, Walsh K. Cardiac-specific deletion of LKB1 leads to hypertrophy and dysfunction. J Biol Chem. 2009;284:35839–35849. 49. de Jong S, van Veen TA, van Rijen HV, de Bakker JM. Fibrosis and cardiac arrhythmias. J Cardiovasc Pharmacol. 2011;57:630–638. 50. Qu Z. Critical mass hypothesis revisited: role of dynamical wave stability in spontaneous termination of cardiac fibrillation. Am J Physiol Heart Circ Physiol. 2006;290:H255–H263. 51.Barth AS, Merk S, Arnoldi E, Zwermann L, Kloos P, Gebauer M, Steinmeyer K, Bleich M, Kääb S, Hinterseer M, Kartmann H, Kreuzer E, Dugas M, Steinbeck G, Nabauer M. Reprogramming of the human atrial transcriptome in permanent atrial fibrillation: expression of a ventricularlike genomic signature. Circ Res. 2005;96:1022–1029. 52. Barth AS, Tomaselli GF. Cardiac metabolism and arrhythmias. Circ Arrhythm Electrophysiol. 2009;2:327–335. 53. Mayr M, Yusuf S, Weir G, Chung YL, Mayr U, Yin X, Ladroue C, Madhu B, Roberts N, De Souza A, Fredericks S, Stubbs M, Griffiths JR, Jahangiri M, Xu Q, Camm AJ. Combined metabolomic and proteomic analysis of human atrial fibrillation. J Am Coll Cardiol. 2008;51:585–594. 54. Ono N, Hayashi H, Kawase A, Lin SF, Li H, Weiss JN, Chen PS, Karagueuzian HS. Spontaneous atrial fibrillation initiated by triggered activity near the pulmonary veins in aged rats subjected to glycolytic inhibition. Am J Physiol Heart Circ Physiol. 2007;292:H639–H648. 55. Ausma J, Coumans WA, Duimel H, Van der Vusse GJ, Allessie MA, Borgers M. Atrial high energy phosphate content and mitochondrial enzyme activity during chronic atrial fibrillation. Cardiovasc Res. 2000;47:788–796. 56. Cha YM, Dzeja PP, Shen WK, Jahangir A, Hart CY, Terzic A, Redfield MM. Failing atrial myocardium: energetic deficits accompany structural remodeling and electrical instability. Am J Physiol Heart Circ Physiol. 2003;284:H1313–H1320. 57. De Souza AI, Cardin S, Wait R, Chung YL, Vijayakumar M, Maguy A, Camm AJ, Nattel S. Proteomic and metabolomic analysis of atrial profibrillatory remodelling in congestive heart failure. J Mol Cell Cardiol. 2010;49:851–863. 58. Hwang JT, Kwon DY, Park OJ, Kim MS. Resveratrol protects ROS-induced cell death by activating AMPK in H9c2 cardiac muscle cells. Genes Nutr. 2008;2:323–326. 59.Zhang Y, Liu Y, Wang T, Li B, Li H, Wang Z, Yang B. Resveratrol, a natural ingredient of grape skin: antiarrhythmic efficacy and ionic mechanisms. Biochem Biophys Res Commun. 2006;340:1192–1199. 60. Nattel S, Carlsson L. Innovative approaches to anti-arrhythmic drug therapy. Nat Rev Drug Discov. 2006;5:1034–1049. 61. Nattel S. From guidelines to bench: implications of unresolved clinical issues for basic investigations of atrial fibrillation mechanisms. Can J Cardiol. 2011;27:19–26. KEY WORDS: atrial fibrillation ◼ cardiomyopathy ◼ cardiac remodeling ◼ myocardial ischemia ◼ potassium channels AMP-Activated Protein Kinase: Potential Role in Cardiac Electrophysiology and Arrhythmias Masahide Harada, Sarah Naomi Nattel and Stanley Nattel Downloaded from http://circep.ahajournals.org/ by guest on May 2, 2017 Circ Arrhythm Electrophysiol. 2012;5:860-867 doi: 10.1161/CIRCEP.112.972265 Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3149. Online ISSN: 1941-3084 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circep.ahajournals.org/content/5/4/860 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Arrhythmia and Electrophysiology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online at: http://circep.ahajournals.org//subscriptions/