Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
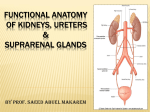
Renal #5 Mon, 03/17/03, 2pm Dr. Rosales Jennifer Uxer for Prateek Chadhaury Page 1 of 6 I. II. Kidneys, Ureters, and Suprarenal Glands Components of the urinary tract Kidneys—a pair of organs, make urine Ureters—transport urine from the kidneys to the urinary bladder Urinary bladder—temporary urine storage Urethra—expels urine from the bladder. In males, it is part of the urinary and reproductive systems. Kidneys A. Functions 1. Maintenance of homeostasis 2. Regulation of fluid and electrolyte balance 3. Production of erythropoietin (hemopoietin, hematopoietin)—stimulates production of RBCs -Enhances erythropoiesis by stimulating formation of proerythroblasts and release of reticulocytes from bone marrow 4. Production of renin (angiotensinogenase) -Renin used to be called a hormone, but it’s actually an enzyme. -Secreted under conditions of hypovolemia by the juxtaglomerular (JG) cells as part of the renin-angiotensin system to elevate blood pressure and elevate blood volume. Angiotensin I is a potent vasoconstrictor. B. Surface Anatomy In the posterior abdominal wall They are primarily retroperitoneal and have no relation to peritoneum. (Secondary retroperitoneal structures were identified in GI, and only their anterior surfaces were covered by peritoneum.) Bean shaped Lateral convex border, and concave medial border. Right kidney is lower than the left due to the liver. C. Development They develop low and ascend to their final position in the posterior abdominal wall. What anatomical structure will arrest the ascent of a “horseshoe kidney” into the retroperitoneal region?—3 Blood Vessels on the abdominal aorta. The 1st is the inferior mesenteric artery. The ascent of normal kidneys is stopped by the suprarenal glands. D. Posterior Relations—listed in the on-line notes 12th rib. Forms the costovertebral angle with the vertebral column. To test for kidney disease, put your palm over the angle and hit the back of your hand with your other fist. Pain is a positive for CVA (costovertebral angle) tenderness—something is wrong with the kidneys. Psoas muscle. When the kidneys are inflamed, this muscle is irritated. To test, have the patient lie on the unaffected side. The affected thigh is extended against resistance. It’s a positive psoas sign if pain is felt. This is also used to test for appendicitis. Renal #5 Mon, 03/17/03, 2pm Dr. Rosales Jennifer Uxer for Prateek Chadhaury Page 2 of 6 Right kidney: diaphragm, costodiaphragmatic recess of the pleura, 12th rib, psoas m., quadratus lumborum m., transversus abdominis m., subcostal n., iliohypogastric n. ilioinguinal n. [N312, N320—3rd ed.] Left kidney: diaphragm, costodiaphragmatic recess of pleura, 11th (left kidney is higher) and 12th ribs, psoas m., quadratus lumborum m., transversus abdominis m., subcostal n., iliohypogastric n., ilioinguinal n. [N312] E. Anterior Relations Right kidney: suprarenal gland, bare area of the liver, 2nd part of the duodenum, right colic (hepatic) flexure [N311, N319—3rd ed.] Left kidney: suprarenal gland, spleen, stomach, pancreas, left colic (splenic) flexure, coils of jejunum F. Coverings (N324, N332—3rd ed) Transverse Section at Level of Body of L.V. 1 1. Fibrous capsule of the kidney—thin, innermost covering; is easily stripped off. It does not divide the kidney into lobes 2. Perirenal fat—thin layer of fat that covers the capsule 3. Renal fascia of Gerota—derived from the transversalis fascia. Encloses the kidney and suprarenal glands. It’s tight at the top and loose inferiorly so that the kidneys descend during deep inspiration. If it were tight inferiorly, it would be painful to breathe deeply. 4. Pararenal fat—part of the fat in the posterior abdominal wall. G. Gross Structure The hilus—found in the medial, concave border. It’s the area where structures enter and exit the organ. The relationship is VAU(A). Renal vein is most anterior. Behind it is the renal artery. The ureter is most posterior. Occasionally, there’s another artery behind the ureter. Look for the direction of the concavity and the way the ureter points. Both ureters point down. Sectioning kidney shows 2 areas: 1. Renal Cortex—outer area, striated, dark brown. Medullary rays, extensions of the medulla into the cortex, located in the cortex and give its striated appearance. 2. Renal Medulla—inner area. Made of the renal pyramids whose bases are directed to the cortex and apices are directed medially toward the hilum. The apex is the renal papilla, where the 1st drops of urine come out. Renal columns, extensions of the cortex into the medulla, are between the renal pyramids. Minor Calyx—start of the excretory duct. Catch the 1st drops of urine and is related to the renal papilla. (Calyx means cup.) Major Calyx—formed by 2 or 3 minor calyces. Renal Pelvis—formed by the merger of the major calyces. It’s the most proximal, dilated portion of the ureter. Renal #5 Mon, 03/17/03, 2pm Dr. Rosales Jennifer Uxer for Prateek Chadhaury Page 3 of 6 Transitional epithelium lines the excretory ducts of the kidneys. Renal sinus—space that holds the vein, artery, and ureter. Filled with perirenal fat to support the structures. Renal hilum—the depression/space. Leads to the renal sinus. H. Blood Supply It’s from the right and left renal arteries. They divide before they enter the kidneys to form the segmental arteries, which are found in the sinus. These supply specific segments of the kidneys, so if a segment is diseased, you only remove that section. This surgery is renal segmentectomy. They are known as lobar arteries as they approach the pyramids. These divide and ascend between the pyramids and are called interlobar arteries. They run on the upper border of the pyramids and are the arcuate arteries. Vasa recta vera, the true straight arteries, come off of the arcuate arteries and enter the pyramids. These give off branches into the medulla and are the interlobular arteries. These are the origin of the afferent arteriole which enters the glomerulus. The efferent arteriole leaves the glomerulus and starts the venous drainage. Vasa recta spurious, the false straight arteries, branch off the efferent arterioles as it leaves the glomerulus. They extend into the medulla and are related to the ascending and descending limbs of Henle and the collecting duct. Their contents flwo in the opposite direction of the contents in the Loop of Henle. This countercurrent causes the concentration of urine. Interlobular vein, arcuate vein, interlobar vein, lobar vein, segmental vein, renal vein, inferior vena cava. NOTE how the efferent arteriole is interposed between the glomerulus (a tuft of capillaries) and the cortical capillary network. Based on this relationship, how would you classify the efferent arteriole as a vessel? As a portal vessel because it can be an artery or vein. Other portal vessels are found in the liver (portal vein) and hypothalamus. What are the arteries of the kidney: anatomical end arteries or functional end arteries? Anatomical end arteries. Anatomical—two unconnected branches Functional—two branches with a small connection that will develop if needed. Renal #5 Mon, 03/17/03, 2pm Dr. Rosales Jennifer Uxer for Prateek Chadhaury Page 4 of 6 abdominal aorta renal a. segmental aa. lobar aa. interlobar aa. arcuate aa. interlobular aa. inferior vena cava renal v. segmental vv. lobar vv. interlobar vv. arcuate vv. interlobular vv. afferent arteriole glomerulus efferent arteriole cortical capillary network I. Lymphatic Drainage: to the nodes related to the renal arteries, the para-aortic nodes. (pre-aortic is for the digestive system) E. Nerve Supply—from the sympathetics and the vagus. They form a plexus of nerves surrounding the renal arteries. II. Ureters A. Function—convey urine from the kidneys to the urinary bladder B. Anatomy Upper ½ is in the abdomen, and lower ½ is in the pelvic cavity. The division between the 2 halves occurs at the external iliac artery and its point of bifurcation of the common iliac artery. The major component of urine is water. External iliac artery is the bridge between the common iliac artery and the femoral artery. Here water passes over the bridge because the ureter passes over here. C. Anatomic Constrictions 1. Ureteropelvic junction (UPJ)—renal pelvis with the ureter 2. Pelvic brim (over external iliac a.)—ureter kinks as it passes over the external iliac artery to enter the pelvic cavity. 3. Ureterovesical junction (UVJ)—enters the urinary bladder. What is the clinical significance of these constrictions? If you’re passing a kidney stone, it can be stuck in 1 of these areas. D. NOTE THE RELATIONSHIP OF THE URETER TO THE UTERINE ARTERY. In females the ureterine artery (branch of the internal iliac artery) passes OVER the ureter. This is important to note so that you don’t transect a ureter. Another ureter injury can occur during catheterization and may create a false passage (a hole) Renal #5 Mon, 03/17/03, 2pm Dr. Rosales Jennifer Uxer for Prateek Chadhaury Page 5 of 6 E. Blood Supply—no specific supply. It comes from branches of blood vessels in the area—from the renal artery, the gonadal artery, the internal iliac artery. F. Lymphatic Drainage—para aortic nodes/ lateral aortic nodes/ lumbar nodes G. Nerve Supply—not specific; acquires innervation as the ureter descends. Upper part is from L1 (junction of the pelvis and the ureter). The branches are the iliohypogastric and ilioinguinal nerves. Therefore the pain of a kidney stone can be referred to the scrotum or the tip of the penis. H. Intravenous Pyelogram (IVP)—inject a water soluble dye. After 15 minutes you can see the excretory ducts of the kidneys. If you don’t see it being excreted, there’s something wrong with the kidneys. III. Suprarenal Glands Have a right and left gland. Be able to identify them by shape. Right is a pyramid/triangle shape. Left is a crescent/half moon shape that extends to the hilum. Both rest on the superior pole of the kidney. A. Blood Supply 3 ARTERIES 1. Inferior phrenic artery superior suprarenal artery 2. Abdominal aorta middle suprarenal artery 3. Renal artery inferior suprarenal artery 1 VEIN Right suprarenal vein inferior vena cava Left suprarenal vein left renal vein B. Nerve supply—celiac ganglia and plexus. It’s mainly sympathetic. C. Suprarenal Cortex Yellowish Derived from mesoderm 3 ZONES 1. Zona glomerulosa mineralocorticoids (aldosterone) -maintenance of fluid and electrolyte balance 2. Zona fasciculate glucocorticoids (cortisol) -control of metabolism of CHO, fats, proteins 3. Zona reticularis sex hormones (androgens: androstenedione, dehydroepiandrosterone) -prepubertal development of sex organs to remember—“the deeper you go the sweeter it gets.” D. Suprarenal Medulla Redish derived from neural crest (neuroectoderm) catecholamines (epinephrine, norepinephrine) secretory cells called chromaffin cells (stored hormones stain with chromium salts) E. Increased Blood Pressure Renal #5 Mon, 03/17/03, 2pm Dr. Rosales Jennifer Uxer for Prateek Chadhaury Page 6 of 6 hypoglycemia, hypoxia, strenuous exercise, stressful emergency situations increased secretory activity greater strength of cardiac contraction acceleration of heart rate redirection of blood flow to muscles and liver general increase in blood pressure IV. Clinical Correlations of Suprarenal Glands A. Cushing’s Syndrome Most common cause of hyperplasia of suprarenal cortex (benign or malignant) Leads to hypersecretion of hormones This, in turn, results in a moon-shaped face, truncal obesity, hirsutism, hypertension B. Addison’s Disease Results from TB or atrophy of adrenal cortex Causes hyposecretion of hormones Results in increased skin pigmentation, muscular weakness, weight loss, hypotension John F. Kennedy had this disease. C. Pheochromocytoma Tumor of adrenal medulla (benign or malignant) Causes hypersecretion of catecholamines Normally, there is no epinephrine in the blood and it’s secreted only when needed. Results in paroxysmal or sustained hypertension (260/160 and asymptomatic)