Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Elbow Trauma
There are 4 essential things to look for in any paediatric elbow x-ray:
Look for fat pads. There are two-anterior and posterior. Visible anterior fat pad is
normal. However, elevated anterior fat pad or any posterior fat pad (either just visible
or elevated) is abnormal and indicates associated haemarthrosis. Commonly due to
occult supracondylar fracture or radial head/neck fracture in children. Fat pad sign is
valid only in a true lateral view with elbow in 90 degree flexion.
*Raised fat pads usually indicate radial head fracture in an adult or supracondylar
fracture in a child
Anterior humeral line. On the lateral view, a line drawn along the anterior surface of
humerus should pass through the middle third of capitellum. In cases of subtle
supracondylar fracture, the line passes thorugh the anterior third or in front of the
capitellum and this is due to the triceps muscle pulling the distal fracture fragment. *If
it doesn’t line up think supracondylar fracture
Radiocapitellar line. On AP and the lateral view, a line drawn through the centre of
the radial neck should pass through the centre of the capitellum. This line is broken in
cases of radial head dislocation or subluxation. Check for accompanying fracture of
ulnar (Monteggia fracture-dislocation).
Ossification centres- have they appeared for given age? Easy to remember mnemonic
CRITOE. I remember it as 2, 4, 6, 8, 10, 12, i.e. the age in years by which the
ossification centre should be there on the film. C-capitellum, R-radial head, I-internal
epicondyle, T-trochlea, O-olecranon, E- external epicondyle.
Useful if your thinking is this an ossification centre or fracture
Suspect avulsion of internal epicondyle if it is absent and there is ossification of the
trochlear
Most common elbow injuries in children
1) Supracondylar fracture
2) Lateral condyle fractures
References
Imaging Cases of the week: 16, 55, 112, 144, 161
Available from: www.emergucate.com
www.radiologymasterclass.co.uk: elbow trauma
www.radiopaedia.org: An approach
Reference text: Grainger & Allison’s Diagnostic Radiology-A textbook of Medical Imaging
Monteggia
Fracture of the ulnar shaft and dislocation of the radial head. Four classifications each
needs open reduction and internal fixation.
Bado classification (direction of the apex of the ulnar fracture fragment points is the
same direction as the radial head dislocation)
I: anterior dislocation of radial head
o classic Monteggia fracture-dislocations
o this type was originally described by Monteggia in 1814
o most common type
II: posterior dislocation of radial head
III: lateral dislocation of radial head
IV: anterior radial head dislocation as well as proximal third ulnar and radial shaft
fractures
Galeazzi
Galeazzi fracture-dislocations consist of fracture of the distal part of the radius with
dislocation of distal radioulnar joint and an intact ulna.
Galeazzi fractures are primarily encountered in children, with a peak incidence of 9-12 years
of age 3.
Mechanism FOOSH
Galeazzi fractures are classified according to the position of the distal radius:
type I: dorsal displacement
type II: volar displacement
These fractures are unstable and operative fixation is usually required to reduce and fix the
radial fracture, and the arm is immobilised in pronation 3-4. The exact mode of fixation
depends on the location of the radial fracture 4:
diaphysis: elastic nail
metaphyseal-diaphyseal junction: plate and screw
distal radius: K-wire
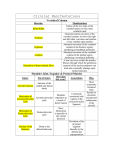
GRIMUS
GRIMUS helps to remember which forearm bone is fractured - and whether the distal
("inferior") or proximal ("superior") part of the bone is involved.
G: Galeazzi
o R: radius
o I: inferior
M: Monteggia
o U: ulna
o S: superior
o