Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
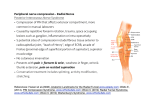
Neil Tarabadkar Department of Pediatric Surgery April 18, 2013 Encompass a spectrum of hypoplasias and dysplasias involving the thumb, wrist, and forearm. • Radial Club Hand • Cleft Hand Deformity • Ulnar Club Hand • Radial Hypoplasia • Absence of the Radius NOT an isolated deformity but a spectrum of dysplasia Bony abnormality of thumb/radius most pronounced • Associated with muscle, nerve, joint and vessel deficiency Hand is usually radially deviated with a short ulna UNKNOWN Upper Limb Development occurs during the first 4-7 weeks of life, along with cardiac, renal, and hematopoeitic systems Several factors have been proposed • Intra-uterine compression • Vascular Insufficiency • Environmental Insults • Maternal Drug Exposure • Genetic Mutations Between 1 in 30,000 and 1 in 100,000 live births Male to Female ratio of 3:2 Bilateral involvement from 38%-58% When unilateral, right upper extremity is involved twice as much as the left Holt-Oram VACTERL Fanconi’s anemia Thrombocytopenia and Absent Radius Class I: Short and mildly dysplastic radius, arising from delayed growth from epiphysis Class II: Growth noticeably diminished secondary to decreased elongation and proximal and distal epiphysis Class III: Partial absence of the radius Class IV: Complete absence of the radius Types II and IV are operative Plays an essential role in functional outcome • Serial splinting and stretching to lengthen taut radial soft tissue • Passive correction (stretching) of wrist deformity • Definitive treatment in pediatrics with mild deformity and • Patients too sick to undergo surgery First performed by Sayer in 1893 Initial surgery performed between 6-12 months Realign/stabilize hand/carpus on distal ulna Distal ulna aligned with long finger metacarpal and stabilized with K-wire, ECU transferred distally, FCU dorsally Goal: maintain deformity correction while optimizing growth, improving digit/wrist motion, enhancing function Hand-Forearm angle is most critical factor High recurrence rate Increased risk of injury to ulnar physis Often need fusion later in life First decribed by Kessler Stretching of the soft tissue via application of a distraction device Goal: controlled and gradual stretching of radial soft tissues Distraction at 1mm/day until passive correction achieved 2nd MTP and Proximal Phalanx can be transferred with a viable physis Vilkki et al and de Jong et all • Average final hand-forearm angle post op 28 degrees • Average wrist motion 83 degrees • Average length of the ulna was 66% of the contralateral side Pin tract infection Vascular complications Inadequate growth of the MTP physis Jong, J. “Changing Paradigms in the Treatment of Radial Club Hand”. Clinical Orthopaedic Surgery. 4:1:36-45. 2011 Mashcke, S. “Radial Longitudinal Deficiency”. JAAOS. 15:1:41-52. 2007 Buffart, L. “Hand function and Activity Performance of Children with Radial Longitudinal Deficiency”. JBJS. 14:90:2408-15. 2008 Bora, William. The Pediatric Upper Extremity.W.B Saunders Publishing. 1986