Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
Increased
HbF
in Sickle
Linked
By Paul F. Milner,
Members
of
sickle
cell
7 large
anemia
hemoglobin
F cells
amounts
of
cell
trait
count
(AS)
than
marked
HbF
and
had
were
also
range.
had
only
HbF
It seems
Ford,
with
HbF
and
in the
remaining
values
in both
F-cell
a factor
small
and
siblings
whereas
a
parents.
the
F cells,
fetal hemoglobin
(a2”y2, HbF)
persists
normally
in a small
proportion
of erythrocytes
called
F cells.’3
Synthesis
of “y-chains
in these cells is
probably
completed
very early
in their
maturation,4
and
HbF
constitutes
only
about
lO%-30%
of the
hemoglobin,
or a mean
of about
4.4 ± 0.3 pg HbF/F
cell.
Population
data
indicate
that,
among
normal
individuals,
F-cell frequency
has a skewed
distribution,
a range
of about
0.5%-7.5%
and
2.5%.’
About
3% of Europeans
cells,”7
and family
studies
have
inherited
as a heterozygous
trait
There
is also good evidence
that
the
‘y#{244}f3-genecluster
and
that
a mode
of about
have more than 8% F
indicated
that this is
for a dominant
gene.7
the gene is linked
to
there
is linkage
disequi-
librium
with the i9S gene,9”#{176}so that,
among
subjects
with sickle
cell trait,
there
is a higher
prevalence
of
increased
F cells than among
subjects
with a normal
hemoglobin
genotype.8”0
Among
proportion
than
patients
of HbF
1% to over
20%,
and
(F retics)
vary from
constant
over time.6
subjects
have normal
majority
it is increased
cell,’1
and
From
lar
in these
and
gia. Augusta.
containing
the
less
HbF
subjects,
there
ofPathology.
the Sickle
Cell
is preferential
Medicine,
Center.
sur-
Cell and Molecu-
Medical
College
of Geor-
GA.
Supported
Lung
reticulocytes
(SS),
from
2% to 55%,6I
The levels remain
Although
about
a quarter
of SS
amounts
of HbF per F cell, in the
to about
a mean of 8 pg HbF/F
the Departments
Biology.
anemia
varies
in part
and Blood
by Grant
Institute.
HL/ilS8from
National
the National
Institutes
ofllealth,
Address
Center,
January
reprint
Medical
0 1 984
6. 1983;
requests
College
by Grune
to Dr.
ofGeorgia.
& Stratton,
0006-497//84/630/-0008$0/.00/0
64
accepted
Inc.
July
Paul
Augusta,
GA 309/2.
the
same
the
55
offspring
it
their
“increased
of
it
greatly
HbF
per
as that
the
result
of
to
of
AA
marrow
similarity
in
Swiss
it
sickle
may
cell
type,
anemia
to the
ultimate
level
if few
F cells
survival
will
amount,
and
this
in most
black
SS
only
of
HbF
were
increase
alone
in any
by
the
can
patients.
HbF
account
by
F cells
contain
for further
increases
in HbF
found,
increased
number
of F cells have this
will
provide,
but a lessening
increase
in red
have
these
et al.’2
similar
patients
have
not
only
that
high
limit
that
HbF
frequently
F reticulocytes
in
of F cells in their
et al.’3 found that
10% HbF
had one
than 0.4% I-IbF, their upper
workers’4
have also observed
might
and if a
property,
rate and an
total
hemoglo-
55 siblings
HbF
levels
and that
correlate
with numbers
parents.
Serjeant
with more than
very
level
more
survival
of the hemolytic
cell count
and
noted
modest
HbF
their
survival
preferential
patient.
a
for the
If the
improved
modulaI-IbF/F
contrib-
preferential
HbF,
levels,
overall
bin.
its
of the
of
55
produced,
account
greatly
their
the
infancy.
additions
of HbF.
Thus,
each or all of these
lions-increased
numbers
of F cells, increased
cell, and preferential
survival
of F cells-may
ute
is
control
vival of F cells in the peripheral
od6’
because
well-known
inhibitory
effect on HbS polymerization
Obviously,
of
hereditary
(HPFH).
HbF
subjects,
hyperplasia
The
that
parents
increased,
heterocellular
suggested
HbF
in AS
greatly
anemia.
hemoglobin
synthesis
F cell
was
in these
increased
of normal
it
gene”
is
in early
is segregating
the
hemolytic
fetal
and
persistent
was
F-cell
persistence
14/16
parent
55 patients
with more
of normal,
and these
the rate of decline
of
HbF in SS infants
over the first 6 yr of life is related
to
the maximum
HbF level in either
parent.
The data we
present
here
indicate
that,
in families
where
55
patients
have
more
than
about
10% of HbF,
this
tendency
teristic
appears
to be inherited
as a dominant
linked
to the f3 gene of one parent.
charac-
Heart,
Bethesda,
MATERIALS
17, 1983.
F. Milner,
was
that
MD.
Submitted
subjects.
with
presence
for
55
associated
and Fred A. Garver
parent,
in the
in
Dover
with sickle
cell
in a hemolysate
of one
suggesting
this
E. Grenett,
is responsible
discussed,
N ADULTS,
with
gene
and
by a Factor
Parent
Hernan
to the
sickle
family,
above
P. Barton,
F cells
had
increased
Betty
One
and
hemoglobin
counts
for
From
families
F-cell
parents
is Determined
linked
of fetal
of the
I of 8 normal
and
that
Janet
levels
both
F cells;
but
Gene
patients
one
higher
family,
at borderline
siblings,
9S
to measure
a much
and
Anemia
immunofluorescence
families,
in one
in HbF
siblings,
“normal”
using
of these
other;
F cells
20
by high
a radloimmunoassay
parents
the
of 14 AS
(AA)
studied
In five
Increase
Seven
I
and
containing
characterized
were
HbF.
to the
D#{246}bler
Leibfarth,
families,
(SS)
(HbF).
to count
Johanna
Cell
Sickle
Cell
Hematologic
using
determined
tified
investigations
a Coulter
Model
were
S cell
by cellulose
by DEAE-cellulose
AND
acetate
METHODS
carried
counter.
out
by standard
Hemoglobin
electrophoresis,
methods
phenotypes
and
fractions
were
quan-
chromatography.
Blood,
Vol. 63, No.
1 (January),
1984:
pp. 64-72
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
INCREASED
HbF
Family
IN
SICKLE
CELL
65
ANEMIA
Studies
Blood
from
multiple
12
patients,
blood
CDE,
group
Jk’Jk’,
drogenase
(G6PD)
TX).
red
was
cell
surface
determined
to
antigens
which
(Helena
there
AB,
II
S
acetate
10
Laboratories,
was
doubt
about
full
from this analysis.
Measurements
HbF
was
alkali
8
measured
in parents
denaturation
munoassay
method
(RIA).”
methods
were
values
measured
1%
low
the
than
by alkali
and
(AD)
At
similar,
below
S
a
dehy-
by cellulose
reagents
in
subjected
P. Glucose-6-phosphate
were
commercial
Families
siblings
and
isoenzymes
were excluded
HbF
for
MNSs,
using
Beaumont,
and
analysis
FyFyb,
electrophoresis
sibship
parents,
of Betke
levels
of
HbF,
denaturation’5
55
and
patients
more
by
S
7
the
the
S
two
reproducible
patients,
S
by the
by a radioim-
results
much
In
HbFAD.
of 55
et al.’5 and
being
HbFRIA
the
siblings
at
HbF
‘6
S
was
S
by a microchromatographic
S
technique
lab Inc.,
(MC)’7
Akron,
patients,
the
but
were
HbF
using commercially
OH).
At the high
gave
HbFMC
considered
measured
values
more
by other
obtained
by elution
liquid chromatography
I
prepared
microcolumns
(Isolevels of HbF found
in some 55
about
20%
accurate
higher
because
chromatographic
from cellulose
(unpublished
than
they
the
and
S
y
S
S.
with
and
acetate
strips
observations).
S
HbFAD,
correlated
procedures”
S
S
S
S
S
by values
S
S
5*5
high-pressure
S
2
S
S
#{149}1
.5
F-Cell
S
Measurements
The
technique
modified
used
as follows.
absorbed
with
divided
HbA,
as
into small
across
frosted
I hr. and
smears
has
the excess,
fixed
to dry,
for 30 mm
were
stained
glycerol.
goat
Diego,
30
washing
mm
at
anti-rabbit
smears
and,
following
examined
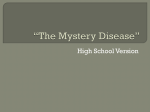
Fig. 1 . Appearance
of F
cells in blood smears visualized
by indirect
immunofluorescence
using antiserum
to HbF
(see
Materials
and
Methods).
(A) Wi I-i ; (B) Wi 11-3; (C)
E 11-9; (D) D 1-2; (E) D 11-3; (F)
D 11-6 (see Fig. 3).
7.2,
wiped
thoroughly
M
away.
PBS,
Molu
for
The
washed
phosphate),
to the smeared
with
the
(Calbiochem-Behring
under
wash,
were
phase-contrast
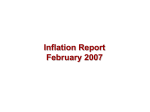
Females
Prenont
Females
Fig. 2.
Percentage
of F cells in immunofluorescent-stainea
blood smears
from 60 unrelated
individuals
with sickle cell trait
(AS). The pregnant
women
were
in the late part of the first or
early part of the second trimester.
areas
smears
ultraviolet
fluorescein-isothiocyanate-
a final
S.
A
made
to dry
for 2 mm,
0.01
applied
y
was
diluted,
were
allowed
circles,
37#{176}Cwith
globulin
were
slides,
pH
batch
smears
(9: 1 , v/v)
serum
and
and exhaustively
was
Blood
glass
(PBS,
the anti-HbF
CA),
The
frozen.
the frosted
saline
and
for
described,’6
and
outside
described3’9#{176}
in rabbits
in acetone:methanol
at 37#{176}C.
After
conjugated
San
previously
on immunologic
in phosphate-buffered
allowed
previously
prepared
aliquots,
circles
were
been
Anti-HbF,
Corp.,
mounted
and
light
using
a Leitz
equipped
with
a Ploem’s
mercury
vapor
lamp.
in
eyepiece
was
by
counted.
When
used
A
to define
the
Dialux
incident
fluorescent
20-EB
Miller
the
fluorescence
illumination
square
microscope
system
graticule
fields
in which
cells
were
and
fluorescent
greater
a lOO-W
placed
than
in
cells
about
one
were
75%,
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
MILNER ET AL.
66
Li)
I-
LACLA
e’NcO
COO)COCO
NNWO)
COCO
LAN
1’)NO
CDC)COCO
IC’)
,-,-o-
NC’4
+1
+
+1
LA
CO
N
O)N’
CO
0)
CO
LOC’)
‘_C4
+1
41
+1
+1
COOCO
C000
tACO
NCO
0’-
‘-N
+1
+1
+1
c’4CON
C’4LA
NCI
+1
+1
+1
LAO
(0’-
COLA
(00
NO)C’)
‘-0)
C0NC’
(0000)
‘
NC,C’)
NCI4
C44
C’NC’)
C1C1
N
0C’)C’)
NC’
C1C’)CS1
C’44
LA
N
CO
LA
+1
+1
NCO
0(0
0)N
‘-
4;
4;
+1
+1
00’-’-
ONN’-
CO
(‘40)
0)N0)
CO
0)
N
COO)’-
(‘4(0
+
+1
,.:
+1
+1
LACO
LAN
+3
NC0
CO(
NC’)
NN
tACO
CON
(00)0)
(0(0
0)(0
CO
0)C1
C,)’+1
‘-
NLAN’
+1
COLA
C’)COCO
CI0)
+1
C’4C0
0000)
ON
‘-0
C’(0
+1
+1
+1
CON
CO
ON
LAO)
,.:
CO
+1
+1
0C’)c’)
+1
‘4’
‘4’
LA
4;
+1
CO
ON
LC
+1
+1
N
+1
qo
Lii
+1
C’)C’)
C’)C’)C’)C’)
+1
u
C)C’)
LA
(‘4
‘*C’)
C’)C’)
C’)
C’)C’)
‘4’
0)0)
c’)O)O)
C’)LALA
C’)C’)C’)
+1
+1
+1
+1
+1
NN
C’)C’)
C’)C’)
C
C
OON
e
C
+1
Cl)
LA
‘N’-’-
00(0
I-.
a.
+1
C’)CiC)
CO
NC0
e
I-
O
LA
LA C)
LA
C’)C’)C’)C’)
NC’)
,+1
4;
4;
4;
+1
c’-q
coo
N
COCO
00
+;
LA
00
+1
0
C’)O)
+i
+1
+1
+1
NO
CO
LAO)
LAO)
Cf)C’)
C’)C’)
C’4
C’)N
C’)N
(“Jo)
COCA
C’)e4
01’)
4;
LA,(0
(0’-
C’)C’)
.C
.v
COC’)O
‘-‘-(0(0
0
C
C
C
>-.
C’)LANN
+
0
+1
0
C’)
LA
‘4’
NC’)CO
+1
Ci0Lt
CO(’40
000
C
+1
4;
+1
0
+1
+1
+1
O
+1
LAO
NO)
NC’)
+1
+1
g0N,
(‘10)
0)0)
O’-OC)
O)N
(‘4
+1
+1
+1
+1
+1
COLA
C’)LA
OCO
N
CO
00)
NC’)
OCO
OCO
0)0)
C
a.
Cl)
Cl)
OCON
CO
CO
0
CO
Lc?
0
NN
C’4
+1
+1
C
C’)
C
+
0
+1
0)
4;
4;
(‘4
+1
+1
CO
CO
NNN
0)LA(’4
C
+1
+1
NCO
0)0
NC’)
C’JN
COOn
CC
‘-
0’-
4-I
N0(’4
NN
C’)NNN
+1
+1
#1
+1
OC’
C’)’-
4;
4;
NOC’)
0(0
NO)
‘COCO
OLA
CO
C’)NN
C’)N
NN
LA’N
NO)
O
NO
C’)N
OOa
00
+i
e
CO
‘‘-‘-NC)
OCOC”I
0
0000)
+1
0
0
0
C
N
x
E
CO
OaOo
+1
C’)
‘4’
+1
N
CO
N
+1
N
C)N
00
N
C’)
00
+1
+1
+1
CO
+141
+1
CO
+1
+1
N0(0
C’)CO
C)N
OCOLACO
(‘4NC’)
0
C)
NC’)
+1
+1
+1
dO
+1
+1
CON’LOLAN
C’4LA
0)’-
O)O
O,O
C’)NC’)
NC’)
C’)C’)
00
00
+1
I
LAC’)C’)
LACOCO
e
.a
+1
C
CO
I-
a
V
+1
N
4;
‘:
+1
+1
+1
C)
LA
LA
CO
+1
N
CO
LO’-C’)
do
dd
000
-H-H
+I+1
LALA
O)(0
+1
N
+1
+1
+1
C’)
+1
+1
O)
C’)
N’-
00)0)
0O)LA
ON
0)0)
O)CO
C’)N
NNN
C’)’-’-
N’-
U.
U.
U.LL
ULL.
LA.
C?C9
CL)
C9
L)C
(‘4C’)
0)CO’CONC’)
‘-0CC
‘4NO
0)0)
C’)N
NN’-’-
C’)C’)C’)’-
LLLu.
.5
C’)LA
00
C
C’)
Ci)-
U
0.0
N
‘-LA
OCO
L(
‘-Ce
COLC)
NLA
N
NN
NN
NC’)
COCO
NC’4
d
c’iL(i
C’)O
NC)
‘-
‘4’O)
‘-C’)
00)
0-
00
od
ON
C’)(’
-JO)?
VC’)
0
.
0
O,4’
LA;
.
DC’)
.0
DC’).
0.0
DC’)
0.0
+1
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
INCREASED
fading
fluorescence
cent
cells
were
were
the
the
smears
from
was
using
in each
counts
were
smear.
is shown
were
were
used
F-cell
for
the
count,
sources.
same
I . The
between
smears
light
by the
in Fig.
60 AS subjects
during
both
Reproducibility
done
2. Blood
not
a problem
counted
scanned
All
67
HbF IN SICKLE CELL ANEMIA
was
observer.
range
the ages
of 15 and
also examined
after
2,000
better
30 are
of
in smears
shown
elution,
2), ages
in Fig.
but
these
enumeration.
RESULTS
Seven
HbFMC
could
group
families
containing
above
10% were studied
be reasonably
antigens
and
20
55
patients
in detail
because
certain,
on the
G6PD
isoenzyme
evidence
patterns,
with
we
of blood
that the
offspring
were
all full siblings.
These
families
intact
at the time of the study,
and the 20 patients
been followed
as outpatients
hematologic
details
are given
Hematologic
values
blood smear
phoresis
results,
were available
family
counts,
for several
in Table
1.
obtained
appearances,
and the
for every
pedigrees,
and percent
years.
F-cell
in any
AA
or AS
comparable
to the siblings
subject
the other
2.2%,
±
whereas
among
1 .8%
subjects
only
although
fractionally
those
above
carriers
arbitrary
family
Their
the
mean
was
that,
given
F cells,
while
all the
55
offspring
more
I
Kindred
(L)s
HbF%
F.cslls
III
HbF %
‘Ia
.0
12.5
0.6
4.5
an
SC
child
(111-4),
Kindred
HbF%
F.c.IIs
JJL-
1.0
9.5
0.4
1.5
18.7
84.0
HbF %
6.5
F.cslls % 23.5
14.3
65.0
AS
AA
0.5
0.6
5.0
1.7
0.3
2.6
%
iitJLI
1.3
8.8
1.1
8.4
1.2
12.5
14.0
65.0
0.5
4.7
15.4
64.0
3.6
3.6
23.0
12.3
I
E
2
A
llE
HbF %
0.2
0.9
F.cSIIs %
2.0
7.8
HbF ‘6
F.c.IIs %
ho
l
II
14.7
72.0
0.3
1.5
14.1
62.0
3.8
12.4
0.5
4.4
-
0.4
5.4
3.5
13.8
112
-
23.4
92.0
-
_____
HbF %
0.8
F.cslls %
6.1
K
20.6
88.0
cI I #{243} 4
0.6
6.9
Pedigrees
22.6
95.0
25.7
96.0
of 7 kindreds
DISd
595
13
0.5
6.7
showing
HbF%
F.cslls %
segregation
2
_____
Wa
0.9
8.6
HbF%
F.cslls %
-
-
-
-
1.1
7.8
12.8
58.0
of the “high
12
13
0.2
3.5
-
2.3
13.5
14
0.3
4.9
0.4
3.0
Is
18.6
78.0
I
DIsdIn
Accldsnt
gene”
L_i
F.cSlIs
‘,‘
3.7
/o
ll#{243}
0.4
3.5
F-cell
Ii
0.1
0.75
Kindred
l[
Kindred
ILj
Kindred
%
113
0.6
6.5
I
2
HbF%
F.cslls
-
HbF%
1
2
Kindred
1
Fig. 3.
have
i
I
Ii ‘#{149}l
HbF %
0.7
F.cslls % 8.0
also
12
lli
0.3
1.2
who
I
1.0
7.5
19.8
92.0
Kindred
HbF %
16.0
F.c&Is % 74.0
and
A
16.5
85.0
-
#{176}/o
F.cslls
0.3
1.8
i.-kI
li
to
a
II, two
and one
an AS
high
12
HbF#{176}/,
F.csIIs %
one
than
of the
families
(Fig. 3) illustrate
this point.
In kindred
Wi, 9 of the 1 1 offspring
were available
and none have died. The four 55 subjects
all have
F-cell
3. It was
decision
rather
(with
had greatly
increased
F cells and
The
following
brief
descriptions
(111-3)
The
F-cell
our
F, generation
AS parent.
value
of the increased
apparent
that, where
F cells and HbF were increased,
the increases
were often greater
in AS offspring
in the
in either
in the
cut-off
value of 7%, one AS parent
(in one
both parents)
and half the AS offspring
had
exception)
10% HbF.
F-cell
counts,
Hb electropercentage
of HbF in lysates
family
member
studied.
The
siblings
(Table
2). In the
had F-cell counts
±
7%,
considered
to have a
count
was
level of HbF.
Of the 4 AS in generation
have HbF and F cells clearly
above “normal,”
of these
subjects
(11-3)
has three
children:
than
as
F, generation
10.6%
F, generation,
it was 4.7%
parental
generation,
several
gene was 10.8%
± 3.2%.
The most striking
finding
were
have
in the
considered
mean
F-cell
among
Counter,
phenotypes,
shown
in Fig.
count
of the families.
Among
subjects
gene for increased
F cells, the
increased
by Coulter
hemoglobin
HbF are
an
abnormally
high was based on the levels reported
in the
literature,3’7”0
and on our own results
in randomly
selected
subjects
between
the ages of 1 5 and 30 yr (Fig.
I 0%.
±
appearance
counted
acid
cells
than
The
of F cells
regard
so nonfluores-
At least
1.0
8.9
17.5
78.0
(hatched)
HbF%
F-cells
linked
%
0.4
5.2
13.5
62.0
to the f
12.8
58.0
locus
in one
parent.
le
20.1
88.0
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
MILNER
68
Table
2.
Segregation
of “High
Total
Examined
Kin&ed
F cells
Increased
F-Cell
Gene”
Among
Siblings
ss
AA
AS
>50%
in one parent
F cells
>7%
F cells
WI
9
4/4
2/4
0/1
E
10
4/4
2/4
0/2
Wa
3
2/2
1/1
L
6
3/3
0/1
?1/2
D
6
2/3
2/2
0/1
G
5
2/2
0/1
0/2
K
3
2/2
0/1
Total
19/20
42
MeanFcells(%
Low F cells
SD)
SD)
±
MeanHbF
(%
in both
±
26
(%
17.2±7.2
4.9 ±
SD)
±
HbF measured by microcolumn
increased
HbF
who does not.
F-cell
tendency
sumably
and
it
increased
gene
the
tendency
gene
from
AA
F-cell
is clear
HbF
the
from
the
borderline
to increased
mother
SS and two of four
In kindred
E,
an
AA
subjects
child
2.2/4.7
±
8.0/3.8
1.8
±
0.65/0.44
±
±
2.0
±
0.73/0.36
0.14
0.16
±
has
F cells.
It appears
and
has
is linked
been
passed
similar
3.6
0.10
0.28
subjects.
and
her,
the
or
F-cell
possibly
gene,
which
her
F cells
appears
do
to have
not
survive
HbF.
that
to the
±
1.6
preferentially.
This family
is extended;
the father
has
an 55 brother
with
3.0%
HbF,
who has four
AS
daughters,
all with normal
HbF and F cells. One of the
mother’s
sisters
has an 55 granddaughter
with
I 7%
a slightly
In kindred
flS
to all four
situation.
0.36
in AS and AA
missed
grand-
mother
1.8
the fS gene
high
pre-
0/2
0/10
3.8±
by RIA
siblings
in generaIn considering
the
F cells
AS offspring.
there
is a
and
(111-2)
her
who
her maternal
and AS
counts.
that
and
and
y in 55
11-2 has not passed
AS daughter
(111-1),
her
father.
The remaining
tion II have normal
parents,
chromatograph
F cells,
Patient
to her
inherits
10.6
1.68
0/14
MeanFcells(%±SD)
HbF
-
71/8
parents
lifamilies
Mean
-
7/14
76 ± 14/23.5
17.4 ± 3.8/6.5
ET AL.
G, the
cells, and her two
16.6%
and 20.1%,
AS offspring
In kindred
The
mother
has
55 daughters
respectively,
increased
HbF
have a mean
but two AA
have not inherited
K, both parents
this
have
and
F
HbF of
and one
characteristic.
an increased
HbF
mother’s
blood was studied
on several
occasions,
and
among
a random
group
of people,
her HbF and F cells
would fall in the upper
part of the normal
distribution.
and F cells. Two 55 offspring
have only moderately
increased
HbF.
If the F-cell
gene is linked
to the flA
locus of the father,
this could explain
its absence
in the
The
AS
contrast
with
her
husband,
however,
is striking,
offspring
who
has
inherited
the
flA gene
from
the
with
parents
low
of
and all four of her 55, and two of three
AS, offspring
available
have increased
F cells.
In kindred
Wa, the two SS and one AS siblings
mother
and the flS gene from
Data
from
large
families
HbF are limited,
but we have
examined
from
the
14 such patients
and some of their siblings.
The results
are summarized
in Table
2, where
they are compared
with
the families
in which
a “high
F-cell
gene”
is
segregating.
have increased
father,
although
F cells, presumably
his HbF
and
inherited
F cells are
barely
above the normal
range.
In kindred
L, both parents
have F-cell
counts
HbF levels bordering
on the upper
limit of normal.
eldest
group
son is probably
is not compatible
illegitimate,
with that
and
The
because
his Jk blood
of his father.
There
are three
SS siblings
with
HbF
levels
among
the
highest
encountered
in black
subjects,
and they could
be homozygous
for an F-cell gene inherited
from each
parent.
But, if this is so, 11-7 has to be a heterozygote,
and 11-1 and 11-3 are examples
of crossovers
of the
F-cell
In
gene during
parental
meiosis.
kindred
D, the mother
clearly
has
increased
cells and has passed
this to two of three
SS and both
AS offspring,
but not to the AA offspring.
The eldest
daughter
may be an example
of a crossover
between
the father.
of 55 subjects
examined
both
The calculated
HbF
per F cell in 55 patients
and
their AS relatives
is compared
in Table
3. F cells from
nonanemic
AS subjects
have a normal
content
of HbF,
no matter
whether
this is calculated
from HbF
measured
by alkali
denaturation
or by RIA.
The
55
patients
have a considerably
higher
content
of HbF per
Table
3.
Calculated
Parents
40)
4.19
±
1.84pg
MCHx
HbF per F Cell
AS Siblings
(n - 14)
(n
F
Mean
3.76
HbF
F cells %
±
1.2pg
(± SD)
AA Siblings
(n - 8)
3.85
±
1.68pg
SS Patients
(n - 20)
7.80
±
0.97
pg
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
INCREASED
HbF
IN
SICKLE
CELL
69
ANEMIA
F cell. This could be an artifact
because
of the method
used for measuring
HbF (microcolumn
chromatography), but, on the other hand, the calculated
mean HbF
per F cell is not very different
from that reported
by
other
workers4’6
Katsura
method.2’
when
measured
directly
using
the
at the extreme
mendelian
autosomal
dominant
inheritance
of a
their
ods?
parents
by biochemical
The recent
investigations
that
there
factor
for increased
HbF and F cells linked
to the f3
locus,
which
segregates
in the families
described
here,
is probably
the same
as that
described
in several
families
reported
in the literature92224
where
small
increases
in HbF
and F cells in one AS parent
have
pearance
age, and
resulted
over
in
much
thalassemia
patient
with
large
ally
larger
offspring,
homozygous
amount
increases
or
of HbF
thesis
is beneficial
gene is probably
lular
hereditary
(HPFH),
which
it may
in
in other
/3-thalassemia
has
55
be different
from
that
F cells,
and
HPFH
described
Weatherall
et
F cells
al.,28’29
in the absence
type heterocellular
Polish
woman
who
25% associated
anemia.3#{176}
An
there
similar
obvious
7.8%
20%
homozygotes
of hemolytic
have
anemia.
Swiss
HPFH
has been documented
in a
had a transient
increase
in HbF to
with
acquired
difficulty
autoimmune
in defining
this
hemolytic
gene
is that
may be an age-related
diminution
in its effect,
to that found
in baboons,3’
making
it difficult
to assess
al.7 had
gation
shown
with
with
from
the nondeletion
in an English
kindred
where
whether
the same
a parent
experience
of Swiss
type
that, in normal
has the gene or not. Zago et
when studying
the segre.
HPFH,
people,
and recently
it has
HbF does decrease
been
with
age.32 It is not clear whether
the high levels of HbF and
F cells reported
for the majority
of SS patients
among
the Shiite
Arabs3335
process
as described
guinity
and
the
can be accounted
here.
The high
increased
F cells
for by the same
level of consan-
in many
outside
We
is a relationship
of HbF
the level
AS
subjects
population
of
120
15 yr of age
distribution,
rate
of disap-
HbF at
whether
(Fig.
and
I 54
female
4). These
we converted
among
55
results
1 yr of
this be
a
patients
are
based
on
for each patient
over
total Hb level has on
each
percent
HbF
to an
result
on
HbF (g/dl)
for each
patient.
The
shown in Fig. 4B. While
curve
accentuates
resulting
distribution
this manipulation
the fact that
most of these
patients
HbF, it does not divide
the population
nor can the distribution
mode,
as would
be
heterocellular
expression
There
is
have very little
into two groups,
be explained
by a three-group
expected
if a recessive
gene
for
HPFH
was
segregating,
in heterozygotes.
is a lot of evidence
from
with
studies
partial
in
both
baboons3”338
and
humans39”#{176} that
erythropoietic
stress
produced
by anemia
induces
increased
“y-chain
synthesis
in early
erythrocyte
precursors.
In both
baboons37
and humans,”#{176} some subjects
respond
with
much
higher
levels
of HbF
than
others,
and
this
appears
to be genetically
determined.
These
studies
have been done
iron-deficiency
from
iron
on animals
anemia,37
with
adult
aplastic
commences
resultant
induced
humans
deficiency39”#{176} or marrow
by cyclophosphamide,39
and
recovering
from
transient
anemia.5
In
sickle
hemolytic
or
recovering
repression
caused
on children
over 6 mo old
erythroblastopenia39’#{176}
or
cell
anemia,
hemolysis
first month
of life, and the
stress
would
be expected
to
increase
7-chain
synthesis
to some extent.
In fact, in
the majority
of 55 infants,
this response
to increasing
hemolysis
is negligible,
and it is mainly
because
of the
relatively
within
the
erythropoietic
longer
S/f3#{176}-thalassemia
than those reported
compartment
postnatal
life.
higher
among
the
infants,
their
in one parent,
male
an
in
absolute
HbF (g/dl),
using the hemoglobin
that blood sample,
and recalculated
mean
that the
increased.
“y-chain
precursors
are, on the whole,
and our patients
are
55
also have
detectable
or within
the normal
range.
looked
at the distribution
of HbFMC
in that population8
would
suggest
that an F-cell gene
with a high frequency,
dominant
in all SS offspring,
would
result
in a high frequency
of 55 with increased
HbF.
However,
the levels
of HbF
in Shiite
SS and
patients
here,
between
in 55
of HbF
this
by Stama-
for black
or morphological
methof Mason
et al.’4 suggest
to have
a
of HbF
Do they
and not
the mean of several
estimations
several
years.
To see what effect
In both SS
HbF
syn-
described
FAD and
heterocellular
100%
5//3#{176}-
in prolonging
red cell survival.
The
similar
to the Swiss type of heterocelpersistence
of fetal
hemoglobin
is found
in about
2% of Europeans,”7
et al.,’#{176}
where
an AS father
F cells had an 55 daughter
by
range
where
a
an unusu-
found
F cells.9’2527
increased
toyannopoulos
HbF and 30%
100%
or
families
and
been
parent
with increased
HbF and
and homozygous
/3-thalassemia,
but
upper
patients.
Lastly,
there
remains
the question
of those
55
patients
with intermediate
levels of F retics and F cells,
who are not entirely
explained
by preferential
survival
of normal
numbers
of F cells.
F-cell
gene,
less well expressed
DISCUSSION
The
those
survival
of the
few
F cells
produced
F-cell
count
and HbF
in peripheral
blood
is
The possession
of a factor
for persistence
of
synthesis
in a greater
number
of red cell
presumably
allows for augmentation
of this
when
hemolytic
anemia
Persistent
reticulocytosis
begins
in our
early
in
patients
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
MILNER ET AL.
70
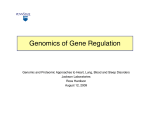
A
0
Male $5 PatIents
Female
SS PatIents
D
U)
C
0
U)
0.
0
HbF
%
E
Male SS Patients
%
Female
SS PatIents
%
U)
C
0
U)
0.
0
<0.2
0.2-
0.4-
0.6-
0.8-
1.2-
1.0-
HbF
is
evidence
because,
of
even
when
continued
F-cell
some cells is insufficient
ture senescence.
These
are
1.6-
1.8-
presumably
high,
the
HbF
in
to prevent
sickling
and premapatients
are also distinguished
by an increased
average
level of HbF per F cell, which
may be the result
of an expanded,
stressed
erythron.
Baboons
made
anemic
tamed
at a hematocrit
and subjected
to further
baric
conditions,
by hemolysis
of about
20%
erythropoietic
maintain
high
and then mainby phlebotomy,
stress by hypo-
F-cell
counts
and
acquire
a higher
HbF
per F cell.4’ To maintain
this
state,
however,
they must be kept in a severely
anemic
or hypoxic
condition,
with
reticulocyte
counts
of
greater
than 50%. The mean reticulocyte
count
in our
patients
was 9.1% (± SE 4.5%),
yet they maintain
a
mean
(±
SE
in the
HbF of 16.9%
(± SE
4.0%).
This is a very
experimental
baboons.
2.0-
2.2-
2.4-
(g/dI)
hemolysis,
counts
1.4-
Fig. 4.
(A) Distribution
of percent
HbF,
measured
by microcolumn
chromatography,
in
1 24 male and 1 54 female
patients
over the age
of 1 5 yr. (B) Distribution
of absolute
level of
HbF (g/dl) in the same 55 subjects.
1.0%) and F cells
different
situation
of 74%
to that
Among
AS
with
lO%-l3%
controlling
those with
subjects
(Fig.
F cells
are
increased
7% F cells
F-cell
might
2), it could
homozygous
be that those
for a gene
production,
in which
case
be heterozygotes.
Among
the homozygotes,
one of the genes
would
have to be
associated
with the chromosome
carrying
the /3” locus,
and half of the AA offpsring
of such subjects
should
have increased
F cells, as well as half the AS offspring.
The data presented
here (Fig. 3), and the frequency
of
increased
F cells among
AA and AS subjects
tested
at
random,3’7”#{176} do not support
increased
F-cell
production
this concept.
If the gene for
is in disequilibrium
with
the flS locus,
however,
homozygotes
more common
among
55 subjects,
of such subjects
would be expected
for it would
be
but both AS parents
to have increased
F
cells, as would
do not support
all their AS offspring.
this, except
possibly
could
inheritance
be that
of two
The
in
genes
present
family
for
data
L. It
increased
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
INCREASED
HbF
IN
F-cell
production
high HbF levels
Arab
55
SICKLE
CELL
71
ANEMIA
in trans
is responsible
reported
in some black
subjects.8
The
levels
of HbF
subjects
reported
here,
however,
heterozygosity
for an increased
the /3 locus of one parent.
It has recently
been found
and
for the very
most Shiite
in most
that
treatment
is associated
with
an
increase
in F cells.
In a sickle
caused
to phlebotomy
to have higher
cell anemia
patient,
F reticulocytes
alone.
resting
5-azacytidine
to increase
per F
high
from
with
‘y-globin
cells.
demethylation
of DNA
genes
recovered
from
bone
Heterocellular
HPFH
of dif-
methylation
in postnatal
/3S
of these
areas
locus could
first, because
more
reproductive
gotes with
survival
have come
the ability
F cells
would
age,
increased
advantage
life.
about
of the
have
in
the
Linkage
by natural
f3 homozygote
favored
to
selecto
survival
to
and second,
because
/3 heterozyF cells might
also have a marginal
in a malarious
environment.
ACKNOWLEDGMENT
We
thank
Bank
to 52%.
10%
associated
with
erythroid
be caused
by mutations
DNA,
which
inhibits
animals
levels.37
treatment
been
ferent
degrees9”#{176}’28’29 may
‘y-globin
gene
associated
make
In the
Such
HbF
has
associated
marrow
the
tion;
f3 homozy5-azacytisynthesis,
anemic
baboons,
there
was an increase
in HbF
cell, and the response
was greatest
in genetically
F-cell
responders
have been shown
to
to
of anemic
baboons42
and human
/3-thalassemia43
and
gotes
with
DNA
methylation
inhibitor,
dine,
causes
a great
increase
in -y-chain
which
of the 55
appear
to be due
F-cell
gene
linked
This
Joyce
M.
Laboratory
invaluable
Larison
of
the
and
her
Medical
technologists
College
of
at the
Georgia
Blood
for
their
assistance.
REFERENCES
I . Marti HR: Normale
und Abnormale
bine. Gottingen,
1963, pp 8 1-89
Boyer
2.
Belding
SH,
TK,
Menschliche
Hemoglo-
Margolet
L, Noyes
AN:
Fetal
acquired
elevations
of HbF.
Blood
46:671,
1975
4. Dover
GJ,
Boyer
SH:
Quantitation
of hemoglobins
within
individual
red cells: Asynchronous
biosynthesis
of fetal and adult
hemoglobin
during erythroid
maturation
in normal subjects.
Blood
56:1082,
1980
5. Dover
GJ,
Boyer
SH,
Bell
WR:
Microscopic
method
for
assaying
F cell production:
Illustrative
changes
during infancy and
in aplastic anemia. Blood 52:664, 1978
6. Dover GJ, Boyer SH: The cellular
distribution
of fetal hemoglobin. Normal
adults and hemoglobinopathies,
in Schneider
RG,
Charache
5, Schroeder
globinopathies.
Medicine,
WA
A Review
vol 40.
(eds):
Human
Hemoglobins
to 1981
. Texas
TX,
University
Galveston,
Reports
and
on
of Texas
Hemo-
Biology
Med
and
MA,
Gunson
H:
53:977, 1979
8. Pembrey
haemoglobin
Saudi
9.
lular
hereditary
saemia
10.
Clegg
WG,
control
JB,
of
Weatherall
F cells
DJ,
in human
ME,
Wood
production
WG,
and
Br J Haematol
WG,
the
sickle
40:415,
Weatherall
Di,
persistence
of
and sickle cell anaemia.
Stamatoyannopoulos
Weatherall
Clegg
foetal
Nature
G,
Wood
Di,
gene
Perrine
in the
RP:
oases
Fetal
of eastern
16.
sickle
Garver
Gravely
and
1:459,
1976
haemoglobin
264:247,
WG,
of heterocelwith
fi thalas-
1976
Papayannopoulou
with
sickle-cell
RJ, Serjeant
decline
disease:
52:455,
FA,
Jones
BE, Serjeant
of fetal
Relationship
haemoglobin
to parental
HbF
1982
CS,
THJ:
quantitation
sickle
18.
man
Baker
MM,
Specific
Altay
G,
percent-
Barton
radioimmunochemical
of hemoglobins
cell
disease.
Schroeder
and
A2
THJ,
Hemoglobin
WA,
Lam
Evans
H, Shelton
determination
of
and/or
J Haematol
C. Am
I 9. Tomoda
Hosoi
BP,
identifi-
F. Am
J
Hematol
JB:
F
Nature
in
EC,
Huis-
microchromatographic
patients
with
of foetal
202:910,
hemoglobins
S
single
F within
Exp
serological
erythrocyte
by immuno-
1964
on hemoglobin
technique.
5: A new
in the
L, Abraham
Quantitative
Y: Demonstration
antibody
1979
1 :33 I , I 976
T: Studies
hemoglobin
3:341,
L, Grussing
hemoglobin
staining.
by fluorescent
Cell
method
erythrocyte.
single
Res
erythrocyte
37:680,
1965
for the detection
Yokohama
Med
of fetal
Bull
15:1 17,
I 964
Horton
hemoglobin
BF, Hahn
DA, Huisman
in apparently
healthy
THJ:
Negroes.
Slight
Acta
increase
Haematol
in fetal
33:3
12,
I965
23.
Th,
Nute PE: A new form of hereditary
persistence
of fetal hemoglobin
in blacks and its association
with sickle cell trait. Blood 46:683,
1975
1 1 . Dover GJ, Boyer SH, Charache
5, Heintzelman
K: Individual
variation
in the production
and survival
of F cells in sickle-cell
disease. N EngI J Med 299:1428,
1978
12. Dover GJ, Boyer SH, Pembrey
ME: F-cell production
in
sickle cell anemia:
Regulation
by genes linked to fl-hemoglobin
locus.Science2ll:144l,
1981
I 3. Serjeant
GR, Serjeant
BE, Mason K: Heterocellular
heredi-
homozygous
17. Abraham
EC, Carver J, D#{246}bler
J, Milner PF, Huisman
THJ:
Microchromatographic
quantitation
of fetal hemoglobin
in patients
22.
Interaction
cell
M, Huisman
cation
1978
JB:
Y, Hayes
Post-natal
WG:
Br J Haematol
20.
Blood
and
I 5. Betke K, Marti HR. Schlicht
I: Estimation
of small
ages of foetal haemoglobin.
Nature 4702: 1877, 1959
O’Sullivan
adults.
KP, Grandison
2 1 . Katsura
Arabia.
Wood
Wood
Genetic
haemoglobin
1977
5, Wood
in homozygous
levels.
fetal
I :795,
Vaidya
fluorescent
7. Zago
of
Lancet
14. Mason
GR,
Branch,
1981, pp 48-54
M,
persistence
hemo-
globin restriction
to a few erythrocytes
(F cells) in normal human
adults.Science
188:361, 1975
3. Wood
WG,
Stamatoyannopoulos
G, Lim G, Nute PE: F-cells
in the adult: Normal values and levels in individuals
with hereditary
and
tary
disease.
of
Martinez
foetal
synthesis?
24.
variant
G, Colombo
haemoglobin:
Nature
Makler
MT.
type
a diffusible
252:735,
of sickle-cell
homogeneously
B: A new
Is
of hereditary
factor
persistence
regulating
‘y-chain
1974
Berthrong
M, Locke
disease
distributed
with
high
within
red
HR,
Dawson
levels
cells.
of foetal
DL: A new
haemoglobin
Br J Haematol
26:5 19,
I974
25.
ME:
26.
JH,
Knox-Macaulay
Thalassaemia
Wood
Barlow
WH,
AM:
HHM,
Weatherall
in the British.
Weatherall
Heterocellular
Di,
Di,
Clegg
Br Med J 3:150,
Clegg
JB,
hereditary
JB,
Pembrey
TJ,
Edwards
1973
Hamblin
persistence
of
fetal
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
72
MILNER
haemoglobin
(heterocellular
thalassaemia.
Br
27.
Rutland
in healthy
Weatherall
Mackenzie
interaction
fi
with
Davies
T: The estimation
by uneven
production
Haematol
of
Boyer
1977
30.
Pawlak
L, Boyer
A2
DJ,
ML,
Clegg
in heterocellular
An
29:256,
A and
Weatherall
WG,
hemoglobin:
distribution
Macrae
WG,
of fetal
IA,
fetal
haemoglobin
of haemoglobin
F and
in homozygotes.
Br
example
of
Huisman
JB,
THJ,
Cartner
hereditary
allelic
exclusion.
tally
foetal
of
Acta
Kozlowska
haemoglobin
Haematol
in a case
43: 1 84,
3 I . DeSimone
Genet
fetal
baboons.
Br J Haematol
ally
Prchal
mild
Hb
of a nonallelic
genic
disorder.
33.
erall
Saudi
45:431,
34.
Wood
Di:
in normal
49: 1 75,
and
Pembrey
ME,
Serjeant
in sickle
with
those
on
10:291,
of
cell
the
example
expressivity
stress.
GR,
of
Acad
the
African
RP,
origin.
Br
Pembrey
Ley
43.
Perrine
in eastern
RP,
Saudi
Wood
Arabia.
WG,
Am
Weatherall
J Hum
Weath-
selectively
of
DJ:
Sick32:26,
J,
in baboons
is
1980
P, Stamatoyannopou-
in response
(Papio
to experimen-
cynocephalus).
WH:
Am
Production
in anemia.
44.
J
of erythro-
J Clin
Invest
63:173,
in
USA
79:4428,
TJ,
P. Hall
Young
G:
Br J Haema-
fetal
J, Anagnou
NS,
Nail
0,
of sickle
hemoglobin
Acad
baboons.
Proc
Natl
GH,
AW:
in a patient
Humphries
5-Azacytidine
with
fl thalasse-
1982
Smith
cell
K, Talbot
anemia
USA
CC
with
production
of DNA
Sci
Keller
P, Nienhuis
synthesis
307:1469,
Dover
NP,
Heller
hypomethylation
Proc
D: 5-Azacytidine
in anemic
1982
‘y-globin
5,
Treatment
L, Zwiers
synthesis
DeSimone
PH,
increased
complex.
expansion.
Bid M, Heller P: Maintenance
of fetal hemogloin the baboon
by prolonged
erythropoietic
hemoglobin
Charache
nonrandom
E, Stamatoyannopoulos
erythroid
1982
increases
5:
Vichinsky
acute
J, Heller
mia. N EngI J Med
J Haematol
Genet
Zinkahm
Th,
60:519,
Turner
Boyer
ME,
Th, Chen
hemoglobin
during
elevations
fetal
Sci
RK,
A comparison
65:224,
production
SH,
fetal
DeSimone
stimulates
of a mono-
Perrine
hemoglo-
1980
Blood
unusu-
1981
anaemia:
anemia
Invest
baboons
Boyer
. DeSimone
42.
with
GJ,
Hb production
bin (HbF)
stressed
siblings
of fetal
1980
contain
tol 44:535,
relationship
erythropoietically
A didactic
gene
Genet
synthesis
cases
anaemia.
1981
G: Two
modifier
J Med
D: Genetic
hemolytic
J Clin
in adult
Papayannopoulou
Fetal
1980
le-fl#{176}
thalassemia
1980
WG,
HbF
Arab
M, Zwiers
$-thalassemia:
Am
persistence
haemolytic
cell disease
56: 187, 1981
I 979
41
J, Stamatoyannopoulos
effect
hereditary
of acquired
P. Bid
levels
homozygous
type
anemia
Dover
that
to acute
of F-cell
8:157,
39.
cytes
1970
J, Heller
between
32.
F: Swiss
5: Sickle
Dis Child
P: Stimulation
PE, Papayannopoulou
induced
40.
AL,
M, Perrine
Arch
Heller
factors.
Acceleration
Hematol
of fetal
J Hum
SI,
response
by genetic
38. Nute
J
R: Inheritance
Am
P. Pembrey
childhood.
J, Bid
hemoglobin
controlled
Schroeder
persistence
John
in early
DeSimone
los G:
Margolet
frequency
F cell
JB, Wood
RP,
Arabs
AL.
bin synthesis
in baboons by hemolysis
and hypoxia.
Proc Natl Acad
Sci USA 75:2937,
1978
37. DeSimone
J, Heller
P, Amsel
J, Usman
M: Magnitude
of the
1975
SH,
Wood
WA,
cellular
Perrine
36.
of fetal
Br J Haematol
persistence
haemoglobins
29:205,
29.
R, Clegg
of hereditary
35.
in Saudi
by radioimmunoassay.
DJ, Cartner
A: A form
characterized
of
ME,
adults
its
1977
1983
28.
the
and
36:461,
PC, Pembrey
haemoglobin
53:673,
HPFH)
J Haematol
ET
around
80:4842,
Jr.,
Moyer
5-azacytidine
and
the
1983
M,
results
is associated
with
‘y-b-fl-globin
gene
From www.bloodjournal.org by guest on June 12, 2017. For personal use only.
1984 63: 64-72
Increased HbF in sickle cell anemia is determined by a factor linked to the
beta S gene from one parent
PF Milner, JD Leibfarth, J Ford, BP Barton, HE Grenett and FA Garver
Updated information and services can be found at:
http://www.bloodjournal.org/content/63/1/64.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.