Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
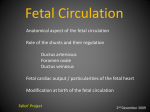
Fetal Physiology Dr Hettiarachchi Anaesthesia & SICU SBSCH- Peradeniya Is uterine blood flow auto-regulated ? Highly muscula r spiral arteries Increasing from ~50 mL/min at 10 weeks’ gestation to >500 mL/min at term Simple diffusion, driven by an oxygen pressure gradient from the mother’s blood to the fetus’s blood Po2 gradient for diffusion of oxygen through the placental membrane is about 20 mm Hg Fetal blood leaving the placenta has a Po2 of only 30 mm Hg Fetal hemoglobin (HbF) can carry 20 to 50 more oxygen than maternal hemoglobin can % Adult haemoglobin Hemoglobin concentration of fetal blood is about 50 % greater than that of the mother Bohr effect The decrease in O2 affinity of hemoglobin when the pH of blood falls Pco2 rises --> P50 rises UNsaturation of hemoglobin Secondary to the decline in the Po2 1–2% unsaturation is due to the rise in Pco2 What is the ‘double Bohr effect’ ? Bohr effect is operative in both the maternal and foetal circulations The double Bohr effect means that the oxygen dissociation curves for maternal HbA and foetal HbF move in opposite directions The foetus requires an increasing oxygen supply as it grows How are these increased oxygen needs met? Increased maternal blood supply to the placenta (Uterine flow increases 20 fold during pregnancy) Increased foetal blood supply to the placenta Presence of HbF which has a higher oxygen affinity than maternal HbA Higher [Hb] concentration in the foetus (40% higher than in adult) Haldane effect Increased capacity of deoxygenated hemoglobin to bind and carry CO2 venous blood carries more CO2 than arterial blood CO2 uptake is facilitated in the tissues, and CO2 release is facilitated in the lungs Fetal cardiovascular adaptations include: 1. Placenta : site of O2 and CO2 exchange 2. Ductus venosus : shunts blood around the liver 3. Foramen ovale : allows O2 -rich blood to bypass the pulmonary circulation 4. Ductus arteriosus (DA): allows right ventricular output to bypass the pulmonary Circulation Neonatal circulation 1. Blood in which of the following vessels normally has the lowest PO2 ? A. Maternal artery B. Maternal uterine vein C. Maternal femoral vein D. Umbilical artery E. Umbilical vein CHANGES IN FETAL CIRCULATION & RESPIRATION AT BIRTH At birth, the placental circulation is cut off and the peripheral resistance suddenly rises Infant becomes increasingly asphyxial and gasps several times Then lungs expand The markedly negative intrapleural pressure (–30 to –50 mm Hg) is created Once the lungs are expanded, the pulmonary vascular resistance falls to less than 20% of the value in utero, and pulmonary blood flow increases markedly. Placental transfusion Sucking action of the first breath plus constriction of the umbilical veins squeezes as much as 100 mL of blood from the placenta Closure of foramen ovale Blood returning from the lungs raises the pressure in the left atrium, Closing the foramen ovale by pushing the valve that guards it against the interatrial septum Ductus arteriosus Constricts within a few hours after birth, producing functional closure Then permanent anatomic closure follows in the next 24–48 h due to extensive intimal Thickening Mechanism Increase in arterial O2 tension Bradykinin, which is released from the lungs during their initial inflation Relatively high concentrations of vasodilators are present in the ductus in utero—especially prostaglandin F2a Prostaglandin synthesis is blocked by inhibition of cyclooxygenase at birth Premature infants - the ductus fails to close spontaneously Closure can be produced by infusion of drugs (e.g., ibuprofen) that inhibit cyclooxygenase Nitric oxide may also be involved in maintaining ductal patency in this setting • • • • • • • 23. Features of Mendelson’s syndrome include: a) urticarial rash b) bronchospasm c) hypoxia d) hypotension e) aspiration of at least 100 ml of gastric contents 23. FTTFF • 38. The placenta: • • a) transports glucose from maternal to fetal blood by facilitated diffusion • b) can synthesise glycogen • c) actively transports oxygen from maternal to fetal blood • d) allows protein molecules to pass from maternal to fetal blood by pinocytosis • e) secretes oestradiol 38. TFFTT