Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
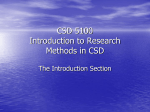
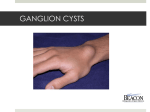
Anesthetic management of a patient with a mediastinal foregut duplication cyst: A case report Aaron R. Gopp, CRNA, MSN Nampa, Idaho 2003 Student Writing Contest Honorable Mention Foregut duplication cysts are rare. There is no mention of this type of mediastinal mass in searches of the anesthesia literature. A 42-year-old woman undergoing preoperative evaluation for elective bilateral breast augmentation was found by chest radiograph to have a mediastinal mass. She was referred for additional evaluation. After thorough radiographic and physical examination, the patient underwent successful resection of a foregut duplication cyst that involved esophageal, right lung, pericardial, and subcarinal tissues. The location of the foregut duplication cyst, its mass effect, and the anatomical structures involved with the cyst T he presence of a mediastinal foregut duplication cyst in an adult can present significant challenges to anesthetic providers. Often the cyst is discovered incidentally, with no previous symptoms described by the patient. Mass location, size, and involvement of adjacent mediastinal structures may have a profound effect on the patient’s hemodynamic and pulmonary function during induction, maintenance of, and emergence from general anesthesia. Comprehensive evaluation of the mass, the adjacent structures, and potential concurrent systemic anomalies is imperative in providing appropriate anesthetic management. This article discusses the occurrence of mediastinal foregut cyst and the evaluation, anatomic, physiologic, and anesthetic management concerns for an adult patient with such a cyst. Case summary A nonsmoking 42-year-old female runner lost more than 10 kg during the preceding year through a regimen of diet and exercise and decided to undergo bilateral breast augmentation. She was an ASA class II patient owing to her long-standing history of arrhythmias and paroxysmal dyspnea and recently developed chest pain. During preoperative evaluation at another facility, a mediastinal mass was discovered on the chest radiograph. The patient elected to postpone the www.aana.com/members/journal/ may present numerous challenges for anesthesia providers. Airway management, arterial cannulation, and central venous access may be difficult. In addition, patients with foregut duplication cysts are at risk for pneumothorax, pneumomediastinum, profound hemorrhage, esophageal injury or rupture, vascular lesions, neurologic injury, gastric aspiration, and cardiovascular collapse due to anatomical disturbances caused by the mass. Comprehensive evaluation and development of an anesthetic plan based on this evaluation will improve patient outcome and help prevent potentially catastrophic complications. Key words: Mediastinal foregut duplication cyst. augmentation surgery pending further evaluation of the mass. At the referral center, she underwent radiologic and pathologic evaluation, including computed tomography (CT) scan and endoscopic fine-needle biopsy. Nine days after the needle biopsy, she came to the emergency department with excruciating chest pain, fever, shortness of breath, tachycardia, anorexia, and extreme dysphagia. She was given intravenous broad-spectrum antibiotics, patient-controlled analgesia for her chest pain, and was scheduled for an emergency exploratory thoracotomy for mass resection and definitive pathological evaluation. Owing to the emergency nature of the surgery, the preanesthetic evaluation was conducted in the preoperative holding area. Respiratory examination revealed bilateral clear lungs, no respiratory distress, and an unremarkable pulmonary function test. An anteroposterior and lateral chest radiograph showed moderate fullness in the right hilum, while the remainder of the thorax, lungs, and heart were unremarkable (Figure 1). Cardiac evaluation confirmed a 20-year history of dysrhythmias, which previously were diagnosed as Wenckebach (second-degree type 1 block), paroxysmal atrial tachycardia, atrial fibrillation, and conduction delay. The patient also described brief periods of random, paroxysmal chest pain, dyspnea, and near syncope associated with arrhythmic episodes. The latter occurred less than once a year and AANA Journal/February 2005/Vol. 73, No. 1 55 Figure 1. Anterior-posterior chest radiograph of patient with embryologic foregut cyst The mass originates at approximately the T4 level, extending inferiorly and into the right mediastinum and pleura at the level of the left atrium. At its widest, the mass measures 3.5 cm anteroposteriorly and 5 cm transversely. The arrow indicates the location of the mass at the lateral right border. (Note: this image is black-white inverted to optimize visualization of anatomical structures.) resolved when she assumed the supine position and drew her knees up to her chest. The patient’s 3 most recent electrocardiograms revealed atrial fibrillation, normal sinus rhythm with right axis deviation, and borderline first-degree atrioventricular block. Echocardiography showed normal chamber function and wall motion and a mediastinal mass radiating from the right side of the esophagus at the T4 level, extending below the carina toward the upper pericardium. The patient’s history also revealed infrequent dysphagia and nausea and vomiting occurring 1 or 2 times a year. Upper gastrointestinal endoscopic ultrasound revealed a “cystic” mass that contained a significant amount of viscous proteinaceous material. Examination of the specimen from transesophageal fine-needle biopsy was unsuccessful in determining the mass pathology. Subsequent swallow studies revealed that no esophageal atresia or communicating fistula was present. A CT scan indicated a right-sided, posterior, elongated mediastinal mass extending downward from the level of the carina to the lower part of the left atrium and located immediately adjacent to the esophagus. The widest diameter, occurring at the level of the proximal right intermediate bronchus, was 3.5 cm in 56 AANA Journal/February 2005/Vol. 73, No. 1 the anteroposterior plane and 5 cm in the transverse plane without infiltration into the lung parenchyma. The CT density indicated the mass to be solid or complex; findings for the remainder of the chest were unremarkable. Radiographic differential diagnoses included neurogenic tumor, lymphoma, and esophageal duplication cyst. The physical examination revealed a physically fit, ASA status II, 168-cm, 54-kg woman with a social drinking history. She was employed as a beautician and often stood for extended periods without difficulty. Before her admission, the patient walked or ran 3 to 6 miles every day on a treadmill and participated in weight training several times each week. The previous surgical and anesthetic history included extraction of wisdom teeth and bilateral radial keratotomy. She had 4 normal vaginal deliveries, 2 with epidural anesthetics. Her family history was noncontributory. Daily medications included digoxin, 0.25 mg; verapamil, 90 mg; and oral contraceptive, multivitamins, and calcium supplements. Allergies included penicillin and sulfa drugs, both of which caused hives. Ciprofloxacin sensitivity resulted in diarrhea when taken for an unrelated upper respiratory infection. Airway evaluation revealed a Mallampati class 2, improving to an Mallampati 1 with phonation, 3finger-breadth thyromental distance, full range of neck motion, wide mouth opening, and intact, native dentition. Her vital signs were as follows: temperature, 37.5°C; SpO2, 96% on room air; pulse, 105 beats per minute; and blood pressure, 106/58 mm Hg. Laboratory test results were as follows: white blood cell count, 12.1 ¥ 109/L; hemoglobin concentration, 9.9 g/dL; hematocrit, 29%; and platelet count, 564 ¥ 109/L. The results of electrolyte and coagulation studies were within normal limits. The patient consented to invasive monitoring, thoracic epidural catheter placement to aid postoperative pain relief, and general anesthesia. Although the patient was extremely anxious, an intravenous line was inserted and sedation administered, and thoracic epidural placement was uneventful. The patient was brought to the operating room, and an arterial line and additional intravenous line were inserted before induction. Radial artery cannulation proved unsuccessful bilaterally. Subsequently, a left brachial artery catheter was inserted. The surgeon requested that the patient be intubated with a 37F left-sided, double-lumen bronchial tube. Following slow induction with 20 mg of etomidate, 325 µg of fentanyl, 5 mg of midazolam, and 6 mg of vecuronium and ventilation with 1.5% isoflurane, 2 attempts were made to insert the double-lumen endo- www.aana.com/members/journal/ bronchial tube. The tube passed easily through the vocal cords and superior trachea but could not be advanced past the T1 level without binding and causing posterior tracheal distortion. To secure the airway, the patient was intubated with a 7.5 oral endotracheal tube. Subsequent fiberoptic bronchoscopy revealed no apparent intratracheal mass or deviation of the trachea or bronchogenic structures. A 35F left-sided, double-lumen tube then was placed successfully, and the position was confirmed with the bronchoscope. An 8F central venous sheath was placed in the right internal jugular vein, and the central venous pressure was monitored; the initial reading was 11 mm Hg. General anesthesia was maintained with 1.2% isoflurane, 100% oxygen, intermittent fentanyl boluses, and vecuronium for the duration of the case. A 120-mg bolus of lidocaine was injected through the epidural catheter during surgical preparations to provide an adjunct to the general anesthetic and minimize narcotic use. Before surgical incision, an 8F Salem sump style nasogastric tube was inserted through the right naris and its position verified by gastric return and auscultation. To facilitate surgery, the right lung was collapsed before incision, and it remained deflated for the duration of the case. Surgical dissection revealed a mass that seemed to emanate from the esophageal wall, was located anterior to the azygos vein, and extended inferiorly from just above the azygos vein downward to the posterior aspect of the pericardium. It extended largely into the right side of the chest and impinged on the right pulmonary vein, resulting in inflammation and erosion. The mass was densely adherent to the adjoining lung, azygos vein, and left portion of the pericardium. The cyst’s wall was very thick and wrapped around the right and left mainstem bronchi. The base of the mass contained a thin area that included the left inferior pulmonary vein. It contained approximately 200 mL of pus within the lumen, and, despite a fistula 2 cm in diameter connecting it to the esophagus, it was, according to the operative report, noncommunicating with the esophagus. Coagulum and the multiple septations of the mass indicated chronicity of the mass and its development from an embryological origin. The mass was dissected from around the pulmonary artery without difficulty, and surgical evaluation confirmed the preoperative diagnosis of esophageal duplication. Surgical pathological evaluation of the dissected mass revealed smooth muscle bundles that formed a well-defined layer within the cystic wall composed of respiratory epithelium and stratified squamous epithelium. Although chronic and acute inflammatory www.aana.com/members/journal/ infiltrates were noted throughout, 1 of the 3 samples contained a small nodule of benign cartilage. The presence of cartilage indicates bronchogenic origin, whereas the smooth muscle layers are consistent with an esophageal duplication. Foregut duplication cystic development will be further examined in the “Case discussion” section. Resection of the left part of the cyst denuded the esophageal mucosa of 7 to 8 cm of circular and longitudinal muscle, allowing visualization of the nasogastric tube in the esophageal lumen. This necessitated the placement of a T tube into the esophagus, which was brought through the right lateral chest wall to allow drainage of secretions. The esophagus was repaired with muscular flaps from the right intercostal musculature. Two Jackson-Pratt drains were placed on either side of the thoracic incision line, and 3 chest tubes were placed around the esophageal defect and externalized from the right lateral side of the chest. Hemodynamic and pulmonary stability were maintained throughout the surgery. The chest was closed, and the patient was extubated immediately postoperatively and transferred to the surgical intensive care unit. Estimated blood loss was 750 mL, urine output was 975 mL, and intraoperative fluid administration included 3,100 mL of crystalloid, 500 mL of colloid, and 3 U of packed red blood cells. Because the patient had a low hemoglobin concentration and hematocrit value preoperatively and significant blood loss was anticipated, the surgical team requested replacement of blood loss with an equal volume of packed red blood cells to optimize oxygen-carrying capacity and hemodynamic function. On arrival to the intensive care unit, a 6-mL bolus of 0.5 % bupivacaine and 10 µg/mL of hydromorphone was given through the epidural catheter. Subsequently, an epidural infusion of the same analgesic mixture was started at 8 mL/h and titrated to effect until its removal 72 hours postoperatively. A postoperative chest radiograph showed small, bilateral pneumothoraces that resolved before chest tube removal. After an uncomplicated 24-hour stay in the intensive care unit, the patient was transferred to the general surgery floor for recovery and rehabilitation. On postoperative day 8, gastrostomy and jejunostomy tubes were inserted under general anesthesia, and the patient was discharged home on postoperative day 16. The patient had no oral intake for nearly 5 months postoperatively due to persistent dysphagia and esophageal dysmotility and had multiple uneventful esophageal dilations under general anesthesia to aid in resolution of the dysphagia. Moreover, she required a cardiac electrophysiology study for AANA Journal/February 2005/Vol. 73, No. 1 57 ablation of aberrant atrial conduction pathways to resolve cardiac dysrythmias and near-syncopal episodes. Case discussion Foregut malformation cysts are uncommon and are quite rare in adults.1-3 The vast majority of mediastinal cystic lesions are diagnosed in infancy or early childhood as a result of symptoms such as dysphagia, vomiting, dyspnea, and other difficulties. In children, foregut malformations make up approximately 11% of mediastinal masses.1 Esophageal duplications make up between 0.5% and 2.5% of esophageal tumors, whereas bronchogenic cysts are more common.2,3 Of all foregut cysts, 25% to 35% are discovered incidentally in adults, and the incidence in men is twice that in women. Postmortem evaluation of esophageal duplication reveals an incidence of 1 in 8,200.3 Mediastinal cysts typically are classified only after comprehensive pathological evaluation. Pathological determination often is difficult, leaving some pathologists to classify them as foregut cysts of aberrant embryological pathology rather than specifying bronchogenic cysts or esophageal duplications. At least 2 pathological classification systems of these foregut cysts are described in the literature.4 Of mediastinal cysts in 27 adults reported by Cioffi et al,2 16 were classified as bronchogenic and 11 as esophageal. Bronchogenic cysts typically are lined with ciliated columnar epithelium, contain cartilaginous material, and may contain mucoid material if they are noncommunicating with the esophagus. Esophageal duplications are classified by the presence of squamous, columnar, pseudostratified, ciliated, or cuboidal epithelium and are adjacent to the esophageal wall.2,4 • Diagnosis and radiologic evaluation. The vast majority of foregut cysts are diagnosed in infancy or early childhood after evaluation of symptoms, including dysphagia, vomiting, dyspnea, and other difficulties.2 In adults, diagnosis of cystic lesions often is incidental after evaluation of routine chest radiographs.2,5 Roughly one third of adults exhibit no symptoms; however, symptoms may include epigastric pain, chest pain, dysphagia, and/or cough.2,6 Chest pain predominates in patients with bronchogenic cyst, whereas dysphagia usually is present only in esophageal duplications.2 Mass location may provide insight into the diagnosis of certain types of embryological cysts. Of the 27 cases reviewed by Cioffi et al,2 10 of 16 bronchogenic cysts were located in the right posterior middle mediastinum.2 In the same study, the vast majority of the esophageal duplication 58 AANA Journal/February 2005/Vol. 73, No. 1 cysts were located in the right posterior inferior mediastinum; however, they also may be located midline in the posterior mediastinum.7 Foregut cysts also have been reported intrapericardially, subdiaphragmatically, and thoracoabdominally.2,8,9 Current radiologic literature recommends evaluation of all mediastinal cysts to determine size, location, and type with magnetic resonance imaging and CT scanning.10-12 Ultrasonography may provide preliminary information; however, additional radiologic studies generally will be required.12,13 Recommendations for transesophageal ultrasonography are contradictory: several authors advocate this method, but others strongly oppose it.2,13-17 Transthoracic echocardiography may indicate cardiac involvement in cystic formations. Further supporting the difficulty in diagnosis, there has been a report of a cystic lesion that initially was diagnosed as a left atrial tumor by chest radiography and transthoracic echocardiography.18 Endoscopic fine-needle aspiration of cysts before surgery remains controversial because it may assist in pathologic evaluation but risks seeding the mass with bacteria,2,19 as apparently happened in the present case. • Embryological development, anatomy, intervention, and pathophysiology. A review of the embryological development of the lungs and esophagus is essential to understanding foregut cysts. The esophagus and trachea initially develop from the ventral wall of the foregut. Esophageal and tracheal separation occurs before 5 weeks’ gestation, and at approximately 5 weeks’ gestation the mucosal and submucosal layers of the trachea and esophagus begin to develop.4,20 Alterations in development at this stage may result in cystic formation (Figure 2). Typically, the distal esophagus elongates first, followed by the proximal esophagus, reaching its full length around 7 weeks’ gestation. The patent lumen develops around 10 weeks. During the same period, the esophageal epithelium changes from stratified columnar to cuboidal to ciliated and, ultimately, to stratified squamous. Sympathetic innervation of the esophagus originates from the celiac plexus and thoracic tree, whereas the vagus nerve provides parasympathetic innervation.20 Corresponding bronchogenic development occurs along the same timeline. Of all esophageal duplications, 60% develop in the lower third, 23% in the upper third, and 17% in the middle third of the esophagus.3 It is the location of the cyst rather than cyst volume that has more of an effect on adjacent intrathoracic structures. Cysts that develop in the upper mediastinum typically have greater mass effect per unit volume than do those in the middle or lower mediastinum.2 This phenomenon www.aana.com/members/journal/ Figure 2. Diagram of embryological development and differentiation of foregut tissues Embryological foregut Esophageal duplication cyst Bronchogenic cyst Triple epithelium cyst Note that the location of cyst origination in the embryological pregut generally defines the pathology and location of cyst present at the end of normal gestation. 6 (Adapted from Hoem et al. ) likely is related to the more rigid nature of structures in upper mediastinum and the limited area for structural movement. Aberrancies in the development or positioning of the foregut during embryological development may result in a myriad of malformations including esophageal stenosis, atresia, diverticula, cysts, and duplications.1,21-23 Because the trachea and esophagus develop from the same foregut, it is not uncommon to have concurrent congenital malformation of the respiratory system and esophageal duplication.11,24-28 As development occurs concurrently with other body systems, foreguts cysts may be associated with other systemic abnormalities such as spinal malformation and cardiac anomalies.29-32 Each of the additional systemic malformations should be evaluated carefully to determine its potential effect on anesthetic administration. A diagnosis of foregut duplication cyst requires surgical intervention. Treatment of choice is complete excision via thoracotomy or thoracoscopy with the typical approach from the right chest to avoid the aortic arch. Thoracoscopic excision is reported to reduce postoperative pain, provide superior cosmetic results, and lead to earlier patient discharge.2,33,34 Nomori et al35 reported continuous esophagoscopic monitoring of video-assisted thoracoscopic surgery, which they www.aana.com/members/journal/ believe maintains better esophageal integrity. Specialized monitoring techniques such as this should be discussed with the surgical team to determine the effects on administering anesthesia. The present patient’s extensive mass was inflamed chronically, which may explain several preoperative symptoms. The location of the mass in the upper mediastinum, T4 to the subcarina, disrupted adjacent structures. These structures are relatively fixed in the upper part of the chest and are compromised easily by a mass occupying the already limited space. In addition, the size of the mass and the subsequent mass effect complicated the patient’s course. The intermittent dysphagia she experienced was a likely result of the displacement and physical disruption of the esophageal musculature, resulting in inadequate peristaltic movements when swallowing. Her 25-year history of cardiac dysrythmias and several near-syncopal episodes coupled with dyspnea were likely the result of impingement (mass effect), acute and chronic inflammations, and direct adherence of the atrial pericardium, the carina, and pulmonary vasculature to the cyst. The acute chest pain, dyspnea, fever, and near syncope after the fine-needle biopsy suggest that the mass was unintentionally seeded with bacteria, a complication noted by Cioffi et al.2 • Anesthetic considerations. General anesthesia is indicated for this procedure; thoracic epidural placement may be used as an intraoperative adjunct and for postoperative pain control. Because cyst location may have significant effects on cardiovascular and pulmonary systems, preoperative euvolemia should be achieved, and general anesthesia methods that optimize cardiovascular and pulmonary function should be used.36,37 Foregut cysts, especially those communicating with the esophageal lumen or containing air, have the potential to dilate or rupture as a result of cross-membrane gas diffusion. Therefore, the use of nitrous oxide should be considered very carefully. Furthermore, preoperative fluoroscopic placement of orogastric or nasogastric tubes should be considered by the anesthesia provider to prevent unintentional tracking into the cystic lumen and unintentional vascular damage. Comprehensive review of radiologic studies will assist the anesthesia provider in evaluating mass effect and in determining the appropriate diameter and length of endotracheal tubes.38 Placement of a doublelumen endotracheal tube, bronchial blocker, or other lung isolation device may be indicated in adults. Because these devices are not commonly available in the appropriate size for pediatric patients, right or left mainstem intubation or bronchial blockade may be AANA Journal/February 2005/Vol. 73, No. 1 59 required.4,33 Awake fiberoptic bronchoscopy should be considered preoperatively to rule out intratracheal mass and to visually evaluate mass effect on the airway structures. Intraoperative transillumination of the esophagus also may be needed to assist the surgeon in maintaining esophageal integrity. Furthermore, provisions for cardiopulmonary bypass may be necessary in the presence of large masses that involve critical structures or when prolonged resection could result in cardiovascular collapse. Pulmonary function studies should be evaluated before surgical resection of potentially involved lung tissues. Anesthesia providers also should conduct a thorough review of all body systems in patients with foregut cyst because the presence of concurrent systemic anomalies, as noted previously, may directly affect anesthetic management. Potential surgical complications with relevance to anesthesia include ligation of the vagus or phrenic nerve, resulting in dysphagia; hemiparesis of the diaphragm; and unilateral or bilateral vocal cord paralysis. Infection, hemorrhage, mixed respiratory complications (iatrogenic or in response to lung isolation), and esophageal dysmotility are other reported complications necessitating standard antimicrobial treatment.39 In addition, gastric prokinetics and histamine-2 blockers or proton pump inhibitors may be used to decrease aspiration risk and to facilitate esophageal healing. Preoperative administration of a nonparticulate antacid may minimize effects of esophageal and gastric contents in the operative area. Conclusion The presence of a mediastinal foregut cyst in adults may present a significant challenge to anesthesia providers. Anesthesia care may range from monitored anesthesia care for preoperative radiologic evaluation to combined regional and general anesthesia for resection. Potential complications include airway difficulties, pulmonary vascular compromise, and cardiovascular collapse. This patient’s anesthetic care was accomplished successfully as a result of incorporating a comprehensive preanesthetic evaluation, including pulmonary, cardiovascular, systemic, and radiologic studies with an understanding of the implications of a mediastinal foregut cyst on anesthetic management. REFERENCES 1. McNally J, Charles AK, Spicer RD, Grier D. Mixed foregut cyst associated with esophageal atresia. J Pediatr Surg. 2001;36:939940. 2. Cioffi U, Bonavina L, De Simone M, et al. Presentation and surgical management of bronchogenic and esophageal duplication cysts in adults. Chest. 1998:1492-1496. 3. Kolomainen D, Hurley PR, Ebbs SR. Esophageal duplication cyst: 60 AANA Journal/February 2005/Vol. 73, No. 1 case report and review of the literature. Dis Esophagus. 1998;11:6265. 4. Nobuhara KK, Gorski YC, La Quaglia MP, Shamberger RC. Bronchogenic cysts and esophageal duplications: common origins and treatment. J Pediatr Surg. 1997;32:1408-1413. 5. Diaz de Liano A, Ciga MA, Trujillo R, Coba F, Oteiza F. Congenital esophageal cysts: two cases in adult patients. Hepatogastroenterology. 1999;46:2405-2408. 6. Hoem D, Odegaard S, Morild I, Viste A. Dysphagia caused by an embryonic triple epithelial duplication cyst. Eur J Surg. 2001;167: 546-547. 7. Hara M, Arakawa T, Ogino H, et al. A case of isolated esophageal cyst in the posterior mediastinum. Radiat Med. 2001;19:161-164. 8. Nelms CD, White R, Matthews BD, Ballinger WE Jr, Sing RF, Heniford BT. Thoracoabdominal esophageal duplication cyst. J Am Coll Surg. 2002;194:674-675. 9. Harvell JD, Macho JR, Klein HZ. Isolated intra-abdominal esophageal cyst: case report and review of the literature. Am J Surg Pathol. 1996;20:476-479. 10. Raymond GS, Logan MP. Congenital thoracic masses: imaging features in the adult. Crit Rev Diagn Imaging. 1997;38:115-205. 11. Lev S, Lev MH. Imaging of cystic lesions. Radiol Clin North Am. 2000;38:1013-1027. 12. Cole TJ, Turner MA. Manifestations of gastrointestinal disease on chest radiographs. Radiographics. 1993;13:1013-1034. 13. Berrocal T, Torres I, Gutiérrez J, Prieto C, Luisa del Hoyo M, Lamas M. Congenital anomalies of the upper gastrointestinal tract. Radiographics. 1999;19:855-872. 14. Faigel DO, Burke A, Ginsberg GG, Stotland BR, Kadish SL, Kochman ML. The role of endoscopic ultrasound in the evaluation and management of foregut duplications. Gastrointest Endosc. 1997;45:99-103. 15. Bhutani MS, Hoffman BJ, Reed C. Endosonographic diagnosis of an esophageal duplication cyst. Endoscopy. 1996;28:396-397. 16. Carerj S, Trifiró MP, Oddo A, Lucisano V, Oreto G. Esophageal duplication cyst: a rare obstacle to transesophageal echocardiography. Echocardiography. 1998;15:601-602. 17. Pocas FC, Salgado M, Cardoso C, Pinho C. Diagnosis of esophageal duplication cysts by endoscopic ultrasonography: report of 3 cases [abstract]. Gastrointest Endosc. 2002;56(suppl): S100. 18. Doi YL, Takata J, Kitaoka H, Matsumura Y, Yabe T. Mediastinal cyst masquerading as left atrial tumour [letter]. Lancet. 1996;348: 5859. 19. Dam JV, Rice TW, Sivak MV. Endoscopic ultrasonography and endoscopically guided needle aspiration for the diagnosis of upper gastrointestinal tract foregut cysts. Am J Gastroenterol. 1992;87: 762-765. 20. Johnson MC. The esophagus. Prim Care. 2001;28:459-485. 21. Jobe BA, Baumann HW, Domreis JS, Sheppard BC. Communicating esophageal duplication with Barrett’s esophagus and high-grade dysplasia. Surgery. 2002;132:112-114. 22. Singh S, Lal P, Sikora SS, Data NR. Squamous cell carcinoma arising from a congenital duplication cyst of the esophagus in a young adult. Dis Esophagus. 2001;14:258-261. 23. Gorenstein A, Serour F, Bujanover Y. Unusual presentation of esophageal communicating duplication in a child. J Pediatr Surg. 1999;34:1430-1431. 24. Kuga T, Inoue T, Sakano H, Zempo N, Oga A, Esato K. Congenital cystic adenomatoid malformation of the lung with an esophageal cyst: report of a case. J Pediatr Surg. 2001;36:E4,1-3. 25. Lee S, Lee L, Park JH, Kim YW, Yang M, Shin DW. Extralobar pulmonary sequestration with an associated cyst of mixed bronchogenic and esophageal type. J Korean Med Sci. 1997;12:567-569. 26. Secil M, Goktay AY, Karabay N, Igci E, Pirnar T. Esophageal dupli- www.aana.com/members/journal/ cation cyst coexisting with Bochdalek’s hernia and polysplenia. Eur Radiol. 1999;9:478-480. 27. Phadke AY, Shah SK, Rajput SL, Bhandarkar PV, Abraham P. Incomplete tubular duplication of the esophagus lined by heterotopic gastric epithelium, presenting in adulthood. Endoscopy. 2000;32:535-536. 36. 37. 28. Kim KW, Kim WS, Cheon JE, et al. Complex bronchopulmonary foregut malformation: extralobar pulmonary sequestration associated with a duplication cyst of mixed bronchogenic and oesophageal type. Pediatr Radiol. 2001;31:265-268. 38. 29. Skandalakis JE, Ellis H. Embryologic and anatomic basis of esophageal surgery. Surg Clin North Am. 2000;80:85-155. 39. 30. Sondheimer JM, Rothenberg S. Clinical quiz: esophageal duplication. J Pediatr Gastroenterol Nutr. 2002;34:290, 301. 31. Porte HL, Massouille DG, Lebuffe GR, Wurtz AJ. A unique congenital mediastinal malformation. Ann Thorac Surg. 2001;71:17031704. 32. Nakao A, Urushihara N, Yagi T, et al. Rapidly enlarging esophageal duplication cyst. J Gastroenterol. 1999;34:246-249. 33. Yim A. Thoracoscopic resection of an esophageal cyst in a 4-yearold girl. Chest. 1996;110:545-546. 34. Yim AP. Video-assisted thoracoscopic resection of anterior mediastinal masses. Int Surg. 1996;81:350-353. 35. Nomori H, Horio H, Imazu Y, Morinaga S, Suemasu K. De-epithelialization for esophageal cyst by video-assisted thoracoscopic sur- www.aana.com/members/journal/ gery monitored by esophagoscopy. Thorac Cardiovasc Surg. 1998; 46:107-108. Holemans JA, Rankin SC. Case report: oesophageal duplication cyst causing left lung collapse and hypoperfusion. Br J Radiol. 1995;68:82-84. Eichmann D, Engler S, Odigs H, Schroeder H, Partsch C. Radiological case of the month: congenital esophageal duplication cyst as a rare cause of neonatal progressive stridor. Arch Pediatr Adolesc Med. 2001;155:1067-1069. Zikri MA, Rice TW. Subcarinal foregut cysts: a unique clinical problem. J Cardiovasc Surg (Torino). 2000;41:137-141. Mahajan RJ, Marshall JB. Severe dysphagia, dysmotility, and unusual saccular dilation (diverticulum) of the esophagus following excision of an asymptomatic congenital cyst. Am J Gastroenterol. 1996;91:1254-1258. AUTHOR Aaron R. Gopp, CRNA, MSN, is a nurse anesthetist at West Valley Medical Center, Caldwell, Idaho, and is currently chief of anesthesia services, 915th Forward Surgical Team, US Army Reserves. At the time this article was written, he was a nurse anesthesia student at the University of Iowa Nurse Anesthesia Program, Iowa City, Iowa. ACKNOWLEDGMENTS I would like to thank Ann Willemsen-Dunlap, CRNA, PhD; Cormac O’Sullivan, CRNA, MSN; and Edward Thompson, CRNA, PhD, for their invaluable guidance and assistance with this article. AANA Journal/February 2005/Vol. 73, No. 1 61