Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
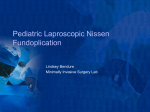
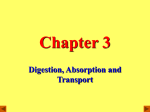
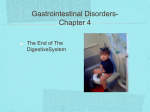
Corrosive Injury of the Upper Gastrointestinal Tract By DR.HISHAM AHMED M.D, Lecturer of General and Pediatric surgery Benha University Hospital/EGYPT Department of Pediatric surgery Leipzig Univesity Hospital/GERMANY 2008 Introduction ► Approximately 80% of caustic ingestions are accidental in children. ► 50% of childhood ingestion cases occur in children less than 4 years of age. ► Alkalis are more frequently swallowed accidentally than acids. The reason is that strong acids cause an immediate burning pain in the mouth. Caustic agents ♦ The most common agents implicated in caustic ingestion are cleaning and dishwasher products and industrial paint strippers. ♦ Alkalis are also contained in hair straighteners and relaxants which may be freely accessible to children in the bathroom environment. ♦ Nowadays alkaline batteries is one of the most common cause of corrosive injuries among children. Location of injury after caustic ingestion Pharynx 10% Whole esophagus 77% Upper 15% Middle 60% Lower 2% Whole Stomach 9% Pyloric antrum 91% 14% Both stomach and esophagus Pathogenesis and Pathology ► The primary difference between alkaline and acidic injury is rapid penetration into the tissue by alkalis. ► Alkalis are producing a “Liquefaction necrosis” with intense inflammation and saponification of the mucousa, submucosa and muscularis of the esophagus and stomach. ► Thrombosis of adjacent vessels results in further necrosis, and bacterial colonization. ► Acidic agents produce a Coagulation necrosis, resulting in a firm protective eschar that delays injury and limits penetration. ► Acidic agents were thought to spare the esophagus and injure the stomach. ► However, ingestion of highly concentrated sulfuric or hydrochloric acid penetrates the esophageal mucosa and produces severe injury in approximately 50% of cases. The severity of injuries depends on multiple factors; ☼ Concentration of the agent ☼ Volume ingested ☼ Duration of contact with the mucosal surfaces ☼ pH of the solution (damage is greatest when the pH is >12) Classification ♦ First degree: Superficial injury produces edema and erythema of the mucosa. ♦ Second degree: Penetration through the submucosa and the muscularis layers. ♦ Third degree: Perforation of the wall of the esophagus or stomach . Clinical Presentation Esophageal and gastric injuries may be present even when the patient has no complaints and examination of the mouth and pharynx is normal . I- Symptoms; * Dyspea * Oral pain * Chest pain * Nausea and Vomiting. II- Signs; * Stridor * Dysphonia or Aphonia * Drooling of saliva * Acute abdomen. * Dysphagia * Odynophagia * Abdominal pain * Hoarseness of voice * Tachypnea * Hematemesis Complications of caustic injuries ☺The severity of complications relates to the depth of injury. ► Superficial mucosal injury is painful but resolves without long term sequelae. ► Deeper caustic injuries result in healing by fibrosis and subsequent stricture. ► Full thickness injury results in perforation and potential fistula formation to either the trachea or in extreme cases the aorta. ☺Development of esophageal carcinoma 15-20 years after the ingestion. Diagnosis A-Esophagogastroscopy ; ♦ The upper gastro-intestinal endoscopy should be performed within the first 24h to assess the extent of injury even in asymptomatic or mildly symptomatic patients. ♦ Esophagoscopy should not be performed in patients with evidence of; * Gastrointestinal perforation. * Significant airway edema, or necrosis. * Hemodynamic un-stability . ☼ Endoscopic grading of corrosive esophageal and gastric burns is: * Grade 0: Normal * Grade I: Mucosal edema and erythema. * Grade II a: Superficial injury. * Grade II b: Superficial injury with limited areas of deeper or circumferential injury. * Grade III a: Small scattered necrotic areas. * Grade III b: Extensive necrosis. Esophagoscopy shows extensive thrombosis of the esophageal submucosal vessels Tissue sloughing and white exudates at the oesophagogastric junction Tissue sloughing and white exudates in the middle of the oesophagus B-Endoscopic ultrasound; Endoscopic ultrasound (EUS) provides better determination of the depth of injury and may prove to be adjunctive or even superior to endoscopy in staging caustic esophageal injury . C-Radiologic studies; 1- Chest and abdominal X ray : * Upright chest and abdominal X-rays may reveal evidence of perforation such as; * mediastinal air * pneumothorax, * pleural fluid * free air under the diaphragm. 2- Computed tumography: ► Computed tumography (CT) of the esophagus and stomach with orally administered contrast is the most sensitive method of detecting early perforation . 3- Contrast study: ► Early esophagogram with water-soluble contrast should be performed at the initial presentation, ♦ If perforation is suspected and ♦ To assess the length of mucosal injury. ► Late esophagogram is usually done 2- 3 weeks after ingestion to determine the presence of strictures. Management A- Early Management; I- Prehospital care II- Emergency department care III- Consultations IV- Medications B- Late Management; I- Esophageal dilatation II- Esophageal stenting III- Esophageal surgery A- Early Management I-Prehospital care; ► Dilution using water or milk may be beneficial if administrated within 30 minutes to remove any adhering particles to the oral or esophageal mucosa . ► Do not use sodium bicarbonate as it generates Co2 and increase the risk of perforation. ► Do not induce emesis ,since vomiting renews the contact of the caustic substance with the esophagus and can contribute to aspiration or perforation if it’s too forceful. ► Do not neutralize the substance by using a weak acid or base. II- Emergency department care; ► Airway control ,Equipment for endotracheal intubation and cricothyrotomy should be readily available. ► Gastric emptying and decontamination ,using nasogastric tube (NGT) and nothing per mouth (NPO). ► Laboratory studies; * PH testing of product * PH testing of saliva * Complete blood count * Urinalysis III- Consultations; ► Obtain a psychiatric consultation for all patients with a history of an intentional ingestion. ► Request surgical consultation if any evidence of perforation exists; ♦ Free air in the peritoneum or mediastinum ♦ Evidence of contrast material extravasation ♦ Evidence of peritonitis ♦ Severe back or retrosternal pain ► Request endoscopic consultation for the following patients: ♦ Small children. ♦ Symptomatic older children. ♦ Patients with altered mental status. IV- Medications; 1- Corticosteroids: Dexamethasone (1mg/kg/day). 2- Collagen synthesis inhibitors: Penicillamine and N-acetylcysteine. 3- Antibiotics: Broad-spectrum antibiotics . 4- H2 receptor blocker : Cimetidine (Tagamet). 5- Parenteral nutrition: Essential when enteral feeding can not be maintained. B- Late Management I- Esophageal dilatation; (only when stricture develops) ♦ Dilatation Should be performed at least once a week with a French catheter 1-2 sizes smaller than the stricture. ♦ Dilatation must be slowly and carefully. ♦ Dilatation must be done under general anaesthesia via a rigid or flexible esophagoscope. ♦ Gastrostomy is indicated in severe burns and when dilatation is difficult II- Esophageal stenting; ♦ Intra-luminal silastic stents under endoscopic guidance in patients with deep circumferential burns. ♦ Twin-tube stenting is helpful in treating caustic lesions and prevent stricture formation. III- Esophageal surgery Surgical intervention is indicated when there is; 1- Complete stenosis with failure to establish a lumen. 2- Stricture longer than 5 cm on radiological assessment. 3- Development of a severe periesophageal reaction or mediastinitis with dilation. 4- Fistula formation. 5- Inability to dilate or maintain the lumen above a 40 French bougie. 6- Patients who refuse prolonged periods of dilation. Surgical Options 1- Esophageal replacement: ► The order of preference for an esophageal substitute is; i- Colon ii- Stomach iii- Jejunum ► An isoperistalitic left transverse and descending colon interposition based on the upper left colic vessels. ► The segment is brought up sub-sternally and anastomosed to the healthy esophagus in the neck, and to the stomach in the abdomen. 2- Sleeve resections of short strictures. 3- Skin tube esophagoplasties VIELEN DANK