Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
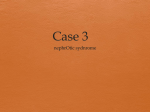
Retinal Capillary Blood Flow Impaired Increase of Retinal Capillary Blood Flow to Flicker Light Exposure in Arterial Hypertension Martin Ritt, Joanna M. Harazny, Christian Ott, Ulrike Raff, Philipp Bauernschubert, Marina Lehmann, Georg Michelson, Roland E. Schmieder Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Abstract—We hypothesized that the increase of retinal capillary blood flow (RCF) to flicker light exposure is impaired in subjects with arterial hypertension. In 146 nondiabetic untreated male subjects with (n⫽50) or without (n⫽96) arterial hypertension, RCF was measured before and after flicker light exposure noninvasively and in vivo using scanning laser Doppler flowmetry. In addition, in a subgroup of 28 subjects, the change of RCF to flicker light exposure was again assessed during parallel infusion of nitric oxide synthase inhibitor N-monomethyl-L-arginine (L-NMMA). The increase of RCF to flicker light exposure was lower in patients with untreated hypertension compared with normotensive subjects when expressed in absolute terms (7.69⫾54 versus 27.2⫾44 AU; P adjusted⫽0.013) or percent changes (2.95⫾14 versus 8.33⫾12%; P adjusted⫽0.023). Systolic (⫽⫺0.216; P⫽0.023) but not diastolic blood pressure (⫽⫺0.117; P⫽0.243) or mean arterial pressure (⫽⫺0.178; P⫽0.073) was negatively related to the percent change of RCF to flicker light exposure, independently of other cardiovascular risk factors. In the subgroup of 28 subjects, the increase of RCF to flicker light exposure was similar at baseline and during parallel infusion of L-NMMA when expressed in absolute terms (20.0⫾51 versus 22.6⫾56 AU; P⫽0.731) or percent changes (7.12⫾16 versus 8.29⫾18%; P⫽0.607). The increase of RCF to flicker light exposure is impaired in arterial hypertension. In the subgroup of the total study cohort, nitric oxide was not a major determinant of the increase of RCF to flicker light exposure. (Hypertension. 2012;60:871-876.) Key Words: retina 䡲 capillary blood flow 䡲 vasodilatory properties 䡲 nitric oxide 䡲 arterial hypertension A rterial hypertension is a major determinant of morbidity and mortality due to cardiovascular complications.1 Reduction in systolic and diastolic blood pressure levels was found to reduce and slow the occurrence of cardiovascular events in subjects with arterial hypertension2; however, blood pressure levels per se might be unreliable indicators of cardiovascular risk in the individual subjects. In arterial hypertension, elevated blood pressure levels lead to structural and functional changes of blood vessels and organ damage, such as retinopathy, thickening of carotid arteries, large artery stiffening, left ventricular hypertrophy, and increased urinary albumin excretion, among others. These subclinical parameters represent intermediate end points that frequently precede major cardiovascular events and indicate the need for aggressive medical blood pressure control in context of individual global cardiovascular risk profile.2 Since the famous work by Keith, Wagener, and Barker,3 several studies have demonstrated the prognostic significance of retinal vascular alterations for predicting morbidity and mortality in subjects with arterial hypertension4–6; however, owing to improvement in patient management, nowadays, grade 3 and grade 4 hypertensive retinopathy are seldom observed, and grade 1 and 2 hypertensive retinopathy reveal low power for predicting cardiovascular events, the classical classification system of hypertensive retinopathy, dating back to the aforementioned work,3 has repeatedly been criticized in the last 2 decades.7,8 In parallel, much research effort has focused on the evaluation of early retinal alterations in arterial hypertension as potential new parameters of hypertensive target organ damage and retinopathy.9–11 Impairment of peripheral vasodilatory properties12,13 represent early vascular changes in arterial hypertension. Of clinical interest, impaired peripheral vasodilatory properties was found to reveal prognostic significance, with respect to adverse cardiovascular outcome in subjects with arterial hypertension.14 Whether vasodilatory properties are impaired in the retinal vascular bed in subjects with arterial hypertension has not yet been examined. Improvement in imaging technology nowadays allows assessment of retinal capillary blood flow noninvasively and in vivo in humans. Moreover, exposure to flicker light was found to increase capillary blood flow in the retinal circulation.15 The mechanisms for the increase of retinal capillary blood flow to flicker light are incompletely understood, but data in healthy subjects indicate that nitric oxide might (at least, in part) be involved.16 In the current study, we hypothesized that the increase of retinal capillary blood flow to flicker light is impaired in Received February 5, 2012; first decision February 27, 2012; revision accepted June 6, 2012. From the Department of Nephrology and Hypertension (M.R., J.M.H., C.O., U.R., P.B., M.L., R.E.S.) and the Department of Ophthalmology (G.M.), University of Erlangen-Nüremberg, Erlangen, Germany; Department of Human Physiology, University of Warmia and Masuria, Olsztyn, Poland (J.M.H.). Correspondence to Dr Roland E. Schmieder, Clinical Research Center, Department of Nephrology and Hypertension, University of ErlangenNüremberg, Ulmenweg 18, 91054 Erlangen, Germany. E-mail [email protected] © 2012 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.112.192666 871 872 Hypertension September 2012 subjects with arterial hypertension. Moreover, we aimed to assess the contribution of nitric oxide on the flicker lightinduced increase of retinal capillary blood flow in a subgroup of the study cohort. Methods Study Design and Study Population Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 This observational study was performed at the Clinical Research Unit of the Department of Nephrology and Hypertension, University of Erlangen-Nüremberg, Germany. Study participants were recruited through advertisements in local newspapers. Patients with arterial hypertension (defined as systolic blood pressure ⱖ140 mm Hg and/or diastolic blood pressure ⱖ90 mm Hg) and normotensive individuals (systolic blood pressure ⬍140 mm Hg and diastolic blood pressure ⬍90 mm Hg) of male gender, between 18 and 75 years of age, were included. Exclusion criteria were history or any present clinical evidence for cardiovascular disease; atrial fibrillation or atrioventricular blockade, grade II or higher; history or current use of any antihypertensive drug or other medication; renal impairment (defined as estimated creatinineclearance ⬍60 mL/min according to the formula by Cockroft and Gault); hepatic disease, diabetes mellitus (defined by fasting glucose ⱖ126 mg/dL or on glucose-lowering medication or history of diabetes mellitus); any form of secondary arterial hypertension; any significant eye disease (including hypertensive retinopathy, grade III and IV), and smoking. Blood pressure was measured in a sitting position, according to World Health Organization criteria, 3⫻, and the average was calculated. Before enrolment in the study, written informed consent was obtained from each participant. The study protocol was approved by the Clinical Investigations Ethics Committee of the University ErlangenNüremberg. The study was conducted in accordance with Good Clinical Practice guidelines and in compliance with the Declaration of Helsinki. Assessment of Parameters of Retinal Vessels Measurement of Retinal Capillary Blood Flow Retinal capillary blood flow was assessed using scanning laser Doppler flowmetry at 670 nm (Heidelberg Engineering). Briefly, a retinal sample of length 2.56 mm (256 points)⫻height 0.64 mm (64 lines)⫻0.30 mm (128 lines: values were averaged for each line and point automatically) was scanned within 2 seconds, at a pixel resolution of 10⫻10 m. The confocal technique of the device ensured that only the capillary blood flow of the superficial retinal layer of 300 m was measured.17 Measurements were performed in the juxtapapillary area of the right eye, 2 to 3 mm temporally to the optic nerve; the average from 3 singular measurements was taken. Analysis of perfusion images was performed off-line with the built-in software automatic full-field perfusion imaging analysis (AFFPIA).18 AFFPIA automatically excludes vessels with a diameter ⬎30 m, underexposed or overexposed pixels, and saccades from the perfusion image, as previously described in detail.18 Thereby, vessel diameters are detected by AFFPIA in reflectivity images, as described previously.19 The mean retinal capillary blood flow was calculated in the area of interest and expressed as arbitrary units. Measurement of Changes of Retinal Capillary Blood Flow to Flicker Light Exposure Retinal capillary blood flow was measured before and after flicker light exposure (10 Hz over 3 minutes; Roland Consult Stasche & Finger GmbH). Flicker light stimulation leads to an increase of retinal capillary blood flow.15 Flicker light exposure has no effects on systemic blood pressure and heart rate, thereby minimizing potential systemic hemodynamic influences on retinal capillary blood flow. Testing Whether the Increase of Retinal Capillary Blood Flow to Flicker Light Exposure is at Least in Part Mediated by Nitric Oxide In the last subjects that could be recruited, we additionally implemented to measured changes in retinal capillary blood flow during parallel infusion of nitric oxide synthase inhibitor N-monomethyl-Larginine (L-NMMA), aiming to test whether the increase of retinal capillary blood flow to flicker light is mediated (at least, in part) by nitric oxide in our subjects. Thereby, at least, in 28 subjects, the change of retinal capillary blood flow to flicker light and the change of retinal capillary blood flow to flicker light during parallel infusion of L-NMMA was measured. In brief, after a resting phase of 15 minutes to ensure that retinal capillary blood flow has returned to baseline levels, L-NMMA (3 mg/kg of body weight; Clinalfa, Bachem AG) was administered intravenously as a bolus infusion over 5 minutes, followed by constant infusion of L-NMMA (0.05 mg/kg body weight per minute) over further 25 minutes. Thus, the total dose of L-NMMA was 3.25 mg/kg body weight. Immediately after bolus infusion of L-NMMA, flicker light stimulation (10 Hz over 3 minutes; Roland Consult Stasche & Finger GmbH) was applied, and retinal capillary blood flow was measured again. If nitric oxide, at least, in part, mediates the increase of retinal capillary blood in response to flicker light, concomitant infusion of nitric oxide synthase inhibitor L-NMMA during flicker light stimulation will lead to a blunted or at least lower increase of retinal capillary blood flow, in response to flicker light. Finally, we infused L-arginine at a dosage of 100 mg/kg body weight over a period of 30 minutes. This was done for safety reasons, as previous examinations from our laboratory have revealed that L-arginine at a dosage of 100/mg/kg body weight reverses the effects of L-NMMA on retinal capillary blood flow. Retinal capillary flow was measured again after L-arginine infusion to ensure that retinal capillary blood flow has returned to baseline levels (data not shown). No dilation of the pupil is required to perform the measurements by the applied techniques, thereby avoiding concomitant pharmacological interaction. All examinations of retinal vasculature were performed in sitting position after 20 minutes of rest, at room temperature, and in daylight conditions between 8 AM and 2 PM but before lunch. The readers (U.H. and S.A.) of retinal vasculature were blinded to the clinical data of the subjects. Statistics All statistical analyses were performed using SPSS software (IBM SPSS Statistics 19). Testing for normal distribution was performed using Kolmogorov-Smirnov tests. Using this test, all parameters were found to reveal a normal distribution. Results are given as mean⫾SD in text and tables. Comparison between groups was performed using the Student t test or, in case of adjustment for possible confounders (including variables that differed with a P value ⬍0.05 or tended to differ with a P value ⬍0.10 between the hypertensive and normotensive group), using univariate analysis of variance. Univariate correlation analyses were performed using Pearson‘s correlation coefficient. Multiple linear regression analyses were performed to determine whether blood pressure and cardiovascular risk factors were independently of possible confounders related to the change of retinal capillary blood flow in response to flicker light. Only 1 parameter per variable group (eg, LDL-cholesterol in the lipid variable group) was eligible to be entered as an independent variable, aiming to avoid statistical error due to collinearity. The independent variables were entered simultaneously (multiple linear regression, enter procedure). A 2-tailed P value ⬍0.05 was considered statistically significant. Results Baseline Clinical Characteristics The clinical characteristics of the study participants, stratified into subjects with arterial hypertension and normotensive controls, are given in Table 1: Subjects with arterial hypertension were older and revealed higher body weight, body mass index, blood pressure levels, heart rate, fasting glucose, and triglyceride levels compared with normotensive patients. Height, high-density lipoprotein (HDL)-cholesterol, lowdensity lipoprotein (LDL)-cholesterol, serum creatinine, and Ritt et al Retinal Vasodilatory Capacity in Hypertension 873 Table 1. Clinical and Retinal Characteristics of the Study Cohort, Stratified Into Subjects With Arterial Hypertension and Normotensive Controls Characteristics Hypertensive Subjects (n⫽50) Normotensive Subjects (n⫽96) 40.5⫾7.8 36.8⫾8.9 0.011 ... P Value P Value Adjusted*/† Clinical characteristics Age (y) Height (cm) 182⫾6.5 182⫾6.0 0.867 ... Weight (kg) 99.5⫾16 92.2⫾18 0.014 ... BMI (kg/m2) 30.0⫾4.9 27.8⫾5.0 0.012 ... Systolic blood pressure (mm Hg) 146⫾8.6 129⫾6.4 ⬍0.001 ... Diastolic blood pressure (mm Hg) 88.4⫾7.0 76.5⫾6.4 ⬍0.001 ... Mean arterial pressure (mm Hg) 108⫾6.2 93.8⫾5.2 ⬍0.001 ... Heart rate (beats/minute) 75.5⫾9.9 71.2⫾10 0.015 ... Fasting glucose (mg/dl) 101⫾16 95.5⫾13 0.028 ... Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Triglycerides (g/dl) 199⫾121 159⫾90 0.027 ... HDL-cholesterol (mg/dl) 50.4⫾13 49.2⫾8.7 0.564 ... LDL-cholesterol (mg/dl) 152⫾34 143⫾39 0.163 ... Serum creatinine (mg/dl) 0.91⫾0.1 0.89⫾0.1 0.212 ... 118⫾22 120⫾20 0.496 ... Retinal capillary blood flow at baseline (ie, before flicker light exposure) (AU) 360⫾89 334⫾83 0.077 0.229 Change of retinal capillary blood flow to flicker light exposure (AU) 7.69⫾54 27.2⫾44 0.021 0.012/0.013 Change of retinal capillary blood flow to flicker light exposure (%) 2.95⫾14 8.33⫾12 0.019 0.016/0.023 2 Estimated creatinine clearance (ml/min/1.73 m ) Retinal characteristics y indicates years; BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein. *P adjusted for variables that differed with a P value of ⬍0.05 between the hypertensive and normotensive group (ie, age, weight, body mass index, heart rate, fasting glucose, and triglyceride levels. †P adjusted for variables that differed with a P value of ⬍0.10 between the hypertensive and normotensive group (ie, age, weight, body mass index, heart rate, fasting glucose, triglyceride levels, and retinal capillary blood flow at baseline (ie, before flicker light exposure). estimated creatinine clearance did not differ between the 2 groups. Baseline Retinal Characteristics and Changes of Retinal Capillary Blood Flow to Flicker Light Exposure The baseline retinal characteristics and changes in retinal parameter to flicker light exposure of the study participants, stratified into patients with arterial hypertension and normotensive controls, are also given in Table 1: Retinal capillary blood flow at baseline (ie, before flicker light exposure) did not differ between the 2 patient groups. The increase of retinal capillary blood flow to flicker light exposure was lower in subjects with arterial hypertension than in normotensive controls, irrespective whether expressed in absolute terms or in percent changes, even after adjustment of the analysis for possible confounders. Univariate Correlation Analysis Between Various Clinical Parameters and the Percent Change of Retinal Capillary Blood Flow to Flicker Light Exposure Systolic blood pressure (Figure A) and mean arterial pressure (r⫽⫺0.171; P⫽0.039) were negatively related to the percent increase of retinal capillary blood flow to flicker light exposure. The negative relationship of diastolic blood pressure to the percent increase of retinal capillary blood flow to flicker light exposure did not reach statistical significance (Figure B). None of the other clinical parameters, including age (r⫽0.002; P⫽0.980), height (r⫽0.115; P⫽0.168), weight (r⫽0.080; P⫽0.337), body mass index (r⫽0.047; P⫽0.572), heart rate (r⫽⫺0.008; P⫽0.924), fasting glucose (r⫽⫺0.005; P⫽0.956), triglyceride levels (r⫽⫺0.053; P⫽0.529), HDL-cholesterol (r⫽⫺0.114; P⫽0.175), LDL-cholesterol (r⫽⫺0.131; P⫽0.117), serum creatinine (r⫽0.076; P⫽0.366) estimated creatinine clearance (r⫽⫺0.007; P⫽0.933) and retinal capillary blood flow at baseline (ie, before flicker light exposure) (r⫽⫺0.150; P⫽0.072) revealed a significant relationship to the percent increase of retinal capillary blood flow to flicker light. Multiple Linear Regression Analysis Assessing the Quantitative Role of Major Cardiovascular Risk Factors in Relation to Each Other on the Percent Change of Retinal Capillary Blood Flow to Flicker Light Exposure Systolic (model 1) but not diastolic blood pressure (model 2) or mean arterial pressure (model 3) was negatively related to the percent increase of retinal capillary blood flow to flicker light exposure, independently of other cardiovascular risk factors (see Table 2). None of the other cardiovascular risk factors revealed such an independent relationship to the percent increase of retinal capillary blood flow to flicker light exposure (see Table 2). 874 Hypertension September 2012 B 60 40 r=-0.214, P=0.010 20 0 -20 -40 110 120 130 140 150 160 170 180 Systolic blood pressure (mmHg) Change of retinal capillary blood flow to flicker light exposure (%) Change of retinal capillary blood flow to flicker light exposure (%) A 60 r=-0.119, P=0.153 40 Figure. A, Relationship between the percent change of retinal capillary blood flow to flicker light exposure and systolic blood pressure. B, Relationship between the percent change of retinal capillary blood flow to flicker light exposure and diastolic blood pressure. 20 0 -20 -40 60 70 80 90 100 110 Diastolic blood pressure (mmHg) Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Assessment of the Contribution of Nitric Oxide on the Increase of Retinal Capillary Blood Flow to Flicker Light Exposure in a Subgroup (nⴝ28) of the Total Study Cohort The clinical and retinal characteristics of these 28 subjects were as follows: age, 38.9⫾5.5 years; height, 181⫾6.3 cm; weight, 110⫾12 kg; body mass index, 33⫾3.9 kg/m2; systolic blood pressure, 135⫾10 mm Hg; diastolic blood pressure, 81⫾7.9 mm Hg; mean arterial pressure, 98.8⫾7.8 mm Hg; heart rate, 74.8⫾9.1 beats per minute; fasting glucose, 101⫾23 mg/dL; triglycerides, 171⫾77 g/dL; HDLcholesterol, 48.6⫾11 mg/dL; LDL-cholesterol, 150⫾36 mg/ dL; serum creatinine, 0.92⫾0.1 mg/dL; estimated creatinine clearance, 126⫾21 mL/min/1.73 m2; and retinal capillary blood flow, 337⫾56 AU. The increase of retinal capillary blood flow to flicker light exposure did not differ compared with the increase in retinal capillary blood flow to flicker light exposure during infusion of L-NMMA when expressed in absolute terms (⫹20.0⫾51 versus 22.6⫾56 AU; P⫽0.731) or percent changes (⫹7.12⫾16 versus 8.29⫾18%; P⫽0.607) in this subgroup of the total study cohort. Discussion The major finding of our study is that the increase of retinal capillary blood flow to flicker light exposure is impaired in subjects with arterial hypertension compared with normotensive controls. Moreover, systolic but not diastolic blood pressure or mean arterial pressure was found to be negatively related to the percent increase of retinal capillary blood flow to flicker light exposure, independently of other cardiovascular risk factors. Thus, the assessment of changes of retinal capillary blood flow to flicker light exposure might be an interesting noninvasive in vivo tool for detection of early vascular changes in arterial hypertension. It might be rational to hypothesize that either constricted vessels with increased vascular resistance in arterial hypertension might be associated with decreased capillary blood flow and to suggest that changes in baseline capillary blood flow before the flicker light exposure may result in altered relative changes in capillary blood flow after the flicker light exposure; however, in our study, retinal capillary blood flow at baseline (ie, before flicker light exposure) did not differ significantly between the hypertensive and the normotensive group. Moreover, neither in univariate correlation analysis nor in multiple linear regression analysis, a significant relationship between retinal capillary blood flow at baseline and the increase of retinal capillary blood flow to flicker light exposure was found. The underlying mechanisms explaining the impaired increase of retinal capillary blood flow to flicker light exposure in our patients with hypertension compared with normotensive controls remains unclear. Reduced production and/or action of vasorelaxing factors such as nitric oxide, endothelial-derived hyperpolarizing factor, and prostacyclin or increased production or activity of vasoconstrictor factors such as prostanoids (endoperoxides, thromboxane A2), superoxide anions, and endothelin increases vascular tone, leads to chronic vasoconstriction of peripheral vessels, and might impair vasodilatory properties in arterial hypertension.20–22 Impairment of peripheral vasodilatory properties were found to represent early vascular changes in arterial hypertension.12,13 Moreover, remodeling of smallresistance arteries and arterioles, which also occurs early in arterial hypertension23 and can be characterized by changes in the wall (media)-to–lumen ratio of these vessels, might also impact on vasodilatory properties. Remodeled small-resistance arteries and arterioles frequently reveal deposition of extracellular matrix proteins (in particular, collagen) and restructuring of smooth muscle cells in their vessel walls, which might lead to embedding of the contracted vessel in a remodeled extracellular matrix and impairment of vasodilatory properties of the vessels in arterial hypertension.24 As small-resistance arteries and arterioles act as major gatekeepers of tissue perfusion, impairment of vasodilatory properties of these vessels might further lead to reduction in the capillary perfusion reserve of corresponding tissue. In line, we had previously found an inverse relationship between wall-to–lumen ratio of retinal arterioles and the increase of retinal capillary blood flow to flicker light exposure in patients with arterial hypertension but not in normotensive controls.25 Another group had observed an inverse relationship between the media-to–lumen ratio of isolated subcutaneous small arteries and arterioles and coronary vasodilatory response to adenosine infusion in patients with arterial hypertension.26 In a subgroup of the total study cohort, concomitant infusion of nitric oxide synthase inhibitor L-NMMA did not reduce the Ritt et al Table 2. Multiple Linear Regression Analysis Assessing the Quantitative Impact of Various Cardiovascular Risk Factors on the Percent Change of Retinal Capillary Blood Flow to Flicker Light Exposure Change of Retinal Capillary Blood Flow to Flicker Light Exposure (%)  Characteristics P Value Model 1 Age (y) 0.055 0.639 BMI (kg/m2) 0.103 0.292 ⫺0.216 0.023 Heart rate (beats/minute) 0.040 0.658 Fasting glucose (mg/dl) 0.035 0.696 LDL-cholesterol (mg/dl) ⫺0.123 0.224 Estimated creatinine clearance (ml/min/1.73 m ) ⫺0.041 0.726 Retinal capillary blood flow at baseline (ie, before flicker light exposure) (AU) ⫺0.064 0.506 Systolic blood pressure (mm Hg) 2 Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Model 2 Age (y) 0.098 0.435 BMI (kg/m2) 0.069 0.484 ⫺0.117 0.243 Heart rate (beats/minute) 0.010 0.908 Fasting glucose (mg/dl) 0.025 0.785 LDL-cholesterol (mg/dl) ⫺0.122 0.235 Estimated creatinine clearance (ml/min/1.73 m2) ⫺0.038 0.750 Retinal capillary blood flow at baseline (ie, before flicker light exposure) (AU) ⫺0.101 0.292 Diastolic blood pressure (mm Hg) Model 3 Age (y) 0.099 0.417 BMI (kg/m2) 0.090 0.361 ⫺0.178 0.073 Heart rate (beats/minute) 0.029 0.751 Fasting glucose (mg/dl) 0.028 0.757 LDL-cholesterol (mg/dl) ⫺0.122 0.234 Estimated creatinine clearance (ml/min/1.73 m2) ⫺0.042 0.723 Retinal capillary blood flow at baseline, i.e. before flicker light exposure (AU) ⫺0.080 0.406 Mean arterial pressure (mm Hg) y indicates years; BMI, body mass index; LDL, low-density lipoprotein. Characteristics under model 1, 2, and 3 are characteristics that were included in that particular model. increase of retinal capillary blood flow to flicker light. This result does not support the hypothesis of a major impact of nitric oxide on the increase of retinal capillary blood flow to flicker light exposure at first glance; however, in contrast to our study, Dorner et al16 reported a reduced increase of major retinal arteriolar diameters in response to flicker light exposure during concomitant infusion of 3 mg/kg body weight of L-NMMA, a dosage comparable to the dosage used in our current study, in a cohort of 12 young (mean⫾ SD age of 25.6⫾2.1 years) healthy, nonsmoking subjects. The reasons for the discrepancy between the 2 studies might be owing to differences in the methodologies used: Dorner et al16 measured changes in major retinal arteriolar diameter in reflexion images (by digital retinal photography), Retinal Vasodilatory Capacity in Hypertension 875 while we measured true changes in perfusion of the retinal capillary bed by scanning laser Doppler flowmetry. Second, Dorner et al16 used a frequency of the flicker light of 8 Hz, while we used a frequency of flicker light of 10 Hz. Previous data indicate that the frequency of flicker light might indeed impact on retinal capillary blood flow response to flicker light exposure.27 Third, Dorner et al16 used a much shorter flicker light duration of up to 64 seconds compared with a 3-minute flicker period in our current study. Furthermore, most of the patients in our substudy revealed cardiovascular risk factors such as arterial hypertension, metabolic syndrome, or obesity that might have resulted in decreased basal nitric oxide activity.20 Thus, to clearly address the role of nitric oxide in the increase of retinal capillary blood flow to flicker light exposure under physiological conditions, a cohort of healthy volunteers who do not reveal any cardiovascular risk factors will need to be examined. Our study has limitations. First, although the readers of retinal vasculature were blinded to the clinical data (including blood pressure levels and history of arterial hypertension, among others), they might have been biased by detecting signs of hypertensive retinopathy, such as focal arteriolar narrowing among others; however, such signs of hypertensive retinopathy might also be detectable in patients with prehypertension7 that, in case of the current study, have been grouped into the normotensive group. Second, owing to inclusion criteria, our study cohort comprised only male subjects. Hormone levels, that potentially impact on microvascular function, differ between women and men.28 Therefore, results of our study might not be extensible to women. Third, all subjects in our current study were white. It cannot be excluded that the impact of blood pressure on the flicker light-induced changes in retinal capillary blood flow might differ between different ethnic groups. Fourth, owing to the cross-sectional design of our study, we can only describe associations but cannot give any information with respect to a causal role. Perspectives We found that the increase of retinal capillary blood flow to flicker light is impaired in subjects with arterial hypertension. Systolic but not diastolic blood pressure or mean arterial pressure was negatively related to the increase of retinal capillary blood flow to flicker light, independently of other cardiovascular risk factors. Thus, the noninvasive measurement of increases of retinal capillary blood flow to flicker light exposure might represent an interesting research and potentially clinical tool to assess early microvascular changes in vivo in arterial hypertension. Acknowledgments We thank U. Heinritz, S. Avendano, I. Fleischmann, S. Pejkovic, I. Birmann, and D. Bader-Schmieder for their excellent technical assistance. Sources of Funding This work was supported by grants from the German Hypertension League and ELAN-Fund of the University of Erlangen-Nüremberg. Disclosures None. 876 Hypertension September 2012 References Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 1. Lopez AD, Meathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–1757. 2. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Erdine S, Kiowski W, Agabiti-Rosei E, Ambrosioni E, Lindholm LH, Viigimaa M, Adamopoulos S, Bertomeu V, Clement D, Farsang C, Gaita D, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O’Brien E, Ponikowski P, Redon J, Ruschitzka F, Tamargo J, van Zwieten P, Waeber B, Williams B. 2007 guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25:1105–1187. 3. Keith NM, Wagener HP, Barker NW. Some different types of essential hypertension: their course and prognosis. Am J Med Sci. 1939;197:332–343. 4. Breslin DJ, Gifford RW Jr, Fairbairn JF II, Kearns TP. Prognostic importance of ophthalmoscopic findings in essential hypertension. JAMA. 1966;195:335–338. 5. Frant R, Groen J. Prognosis of vascular hypertension; a 9 year follow-up study of 418 cases. Arch Intern Med (Chic). 1950;85:727–750. 6. Palmer RS, Loofbourow D, Doering CR. Prognosis in essential hypertension: eight year follow-up study of 430 patients on conventional medical treatment. N Engl J Med. 1948;239:990–994. 7. Wong TY, Mitchell P. Hypertensive retinopathy. N Engl J Med. 2004; 351:2310–2317. 8. van den Born BJ, Hulsman CA, Hoekstra JB, Schlingemann RO, van Montfrans GA. Value of routine funduscopy in patients with hypertension: systematic review. BMJ. 2005;331:73. 9. Wong TY, Knudtson MD, Klein R, Klein BE, Meuer SM, Hubbard LD. Computer-assisted measurement of retinal vessel diameters in the Beaver Dam Eye Study: methodology, correlation between eyes, and effect of refractive errors. Ophthalmology. 2004;111:1183–1190. 10. Hughes AD, Martinez-Perez ME, Jabbar AS, Hassan A, Witt NW, Mistry PD, Chapman N, Stanton AV, Beevers G, Pedrinelli R, Parker KH, Thom SAM. Quantification of topological changes in retinal vascular architecture in essential and malignant hypertension. J Hypertens. 2006;24:889–894. 11. Harazny JM, Ritt M, Baleanu D, Ott C, Heckmann J, Schlaich MP, Michelson G, Schmieder RE. Increased wall: lumen ratio of retinal arterioles in male patients with a history of a cerebrovascular event. Hypertension. 2007;50:623–629. 12. Panza JA, Quyyumi AA, Brush JE Jr, Epstein SE. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension. N Engl J Med. 1990;323:22–27. 13. Ghiadoni L, Taddei S, Virdis A, Sudano I, Di Legge V, Meola M, Di Venanzio L, Salvetti A. Endothelial function and common carotid artery wall thickening in patients with essential hypertension. Hypertension. 1998;32:25–32. 14. Perticone F, Ceravolo R, Pujia A, Ventura G, Iacopino S, Scozzafava A, Ferraro A, Chello M, Mastroroberto P, Verdecchia P, Schillaci G. Prognostic significance of endothelial dysfunction in hypertensive patients. Circulation. 2001;104:191–196. 15. Michelson G, Patzelt A, Harazny J. Flickering light increases retinal blood flow. Retina. 2002;22:336–343. 16. Dorner GT, Garhofer G, Kiss B, Polska E, Polak K, Riva CE, Schmetterer L. Nitric oxide regulates retinal vascular tone in humans. Am J Physiol Heart Circ Physiol. 2003;285:H631–H636. 17. Michelson G, Schmauss B, Langhans MJ, Harazny J, Groh MJ. Principle, validity, and reliability of scanning laser Doppler flowmetry. J Glaucoma. 1996;5:99–105. 18. Michelson G, Welzenbach J, Pal I, Harazny J. Automatic full field analysis of perfusion images gained by scanning laser Doppler flowmetry. Br J Ophthalmol. 1998;82:1294–1300. 19. Michelson G, Wärntges S, Baleanu D, Welzenbach J, Ohno-Jinno A, Pogorelov P, Harazny J. Morphometric age-related evaluation of small retinal vessels by scanning laser doppler flowmetry. Retina. 2007;27: 490–498. 20. Deanfield JE, Halcox JP, Rabelink TJ. Endothelial function and dysfunction: testing and clinical relevance. Circulation. 2007;115: 1285–1295. 21. Shimakawa H. Endothelial dysfunction in hypertension. J Atheroscler Thromb. 1998;4:118–127. 22. Vanhoutte PM. Endothelial dysfunction in hypertension. J Hypertens Suppl. 1996;14:S83–S93. 23. Park JB, Schiffrin EL. Small artery remodeling is the most prevalent (earliest?) form of target organ damage in mild essential hypertension. J Hypertens. 2001;19:921–930. 24. Intengan HD, Schiffrin EL. Vascular remodeling in hypertension: roles of apoptosis, inflammation, and fibrosis. Hypertension. 2001;38:581–587. 25. Ritt M, Harazny JM, Ott C, Raff U, Lehmann M, Michelson G, Schmieder RE. Influence of blood flow on arteriolar wall-to-lumen ratio in the human retinal circulation. Microvasc Res. 2012;83:111–117. 26. Rizzoni D, Palombo C, Porteri E, Muiesan ML, Kozakova M, La Canna G, Nardi M, Guelfi D, Salvetti M, Morizzo C, Vittone F, Agabiti Rosei E. Relationships between coronary flow vasodilator capacity and small artery remodelling in hypertensive patients. J Hypertens. 2003;21:625–631. 27. Riva CE, Logean E, Falsini B. Visually evoked hemodynamical response and assessment of neurovascular coupling in the optic nerve and retina. Prog Retin Eye Res. 2005;24:183–215. 28. Mendelsohn ME, Karas RH. Molecular and cellular basis of cardiovascular gender differences. Science. 2005;308:1583–1587. Novelty and Significance What Is New? ● The increase of retinal capillary blood flow to flicker light exposure, assessed by scanning laser Doppler flowmetry, is lower in hypertensive compared to normotenisve subjects and negatively related to systolic blood pressure, independently of possible confounders. ● Assessment of changes in retinal capillary blood flow to flicker light exposure by scanning laser Doppler flowmetry allows detection of early microvascular changes in hypertension. What Is Relevant? Summary Our current study introduces a new, safe, and elegant noninvasive in vivo tool for detection of early microvascular changes in hypertension, which might be of great interest for future research, as well as patient management. Impaired Increase of Retinal Capillary Blood Flow to Flicker Light Exposure in Arterial Hypertension Martin Ritt, Joanna M. Harazny, Christian Ott, Ulrike Raff, Philipp Bauernschubert, Marina Lehmann, Georg Michelson and Roland E. Schmieder Downloaded from http://hyper.ahajournals.org/ by guest on April 28, 2017 Hypertension. 2012;60:871-876; originally published online July 9, 2012; doi: 10.1161/HYPERTENSIONAHA.112.192666 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2012 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/60/3/871 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/