Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
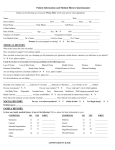
MEDICAL HISTORY RECORD Name: _______________________________________________ Home #: __________________________Cell#: ________________________ Address: ________________________________________ Apt#:_________ City:___________________ State:______ Zip Code: ___________ Birth Date: _____/______/_______ Age:______ Email: _______________________________________________ Marital Status:____________ SSN:_____-_____-_______ Employer:__________________________ Occupation:_______________________ Work#:____________________ Vision Insurance: _______________________________________________ Primary S.S.N./ID#: ______________________________________ Medical Insurance: ______________________________________________ ID#:___________________________________________________ Personal Medical Information: Which of the following conditions do you experience? Please check all that apply □ High Blood Pressure □ Neuropathy □ Depression □ Cancer Type _____________________ □ Diabetes Type _______ □ Seasonal Allergies □ Gastrointestinal Disease □ Lupus □ Heart Disease □ Arthritis □ Genitourinary Disease □ Fibromyalgia □ Asthma □ Skin Conditions □ Thyroid □ Other __________________________ Date of your last routine eye exam: ________________________ Where? ______________________________ Do you have allergic reactions to medications or other substances? □ Yes □ No If yes, please list: ___________________________________________________________________________________________________ Name of Family/Primary Doctor _____________________________________________ Phone/Fax: ________________________________ Please check Yes or No Do you smoke? □ Yes □ No Do you drink alcohol? □ Yes □ No Are you pregnant or nursing? □ Yes □ No □ N/a Please list any current medications: _____________________________________________________________________________________ Do you have any family history of any of the following? If Yes, please check all that apply □ High Blood Pressure □ Macular Degeneration □ Cataracts □ □ Diabetes Retinal Detachment □ □ Other Glaucoma Please explain any boxes you have checked ____________________________________________________________________________ Do you have any of the following? If Yes, please check all that apply □ Dry Eyes □ Eye Surgeries □ Cataracts □ Iritis/Uveitis □ Eye Injuries □ Blurred Vision □ Lazy Eye □ Eye Infection □ Corneal Abrasion □ Diabetic Eye Disease □ Macular Degeneration □ Glaucoma □ Wear Glasses □ Retinal Detachment □ Wear Contacts Brand/Type: Whom may we thank for referring you? ____________________________________________________________________________________ I hereby assign all vision and medical benefits to which I am entitled and any other plans to Dr. Paul Tachau and Associates of Accent on Vision. I hereby authorize said assignee to release all information necessary to secure the payment. I agree that I am responsible for my bill regardless of whether my insurance pays or denies my claim. I understand that there are no refunds for examinations/treatment services or material purchases including eyeglasses, and am aware that vision insurances do not cover medical or surgical treatment of eye injury or disease (allergy, dry eye, glaucoma, etc.) and that the reason for my visit today will dictate which services will be rendered and which payer will be billed. All copays and balances are due at check out on day of service (deductibles also apply), and balances older than 45 days may be subject to additional charges and interest. I am also acknowledging that I have reviewed Accent on Vision’s Notice of Privacy Practices. Patient Signature (or personal representative): _________________________________________________ Date: ______________ Relationship to Patient (if signed by a personal representative of patient): _______________________________________________ Optomap Digital Retinal Imaging Our doctors are concerned about retinal diseases such as macular degeneration, glaucoma, retinal detachments, and diabetic retinopathy; all of which can lead to partial loss of vision or blindness. Additionally, systemic diseases such as diabetes and high blood pressure can be detected with a retinal examination. Eye exams with retinal evaluations can help you safeguard both your eyesight and general health. The Optomap Digital Retinal Imaging allows us to thoroughly evaluate your internal eye health with dramatically improved precision that includes a depth in the retina not seen with regular dilation. The doctor strongly recommends that all patients have this procedure performed annually. It is especially important for people who have: Headaches Diabetes High Blood Pressure High Cholesterol Family history of Glaucoma, Macular degeneration, and/or blindness Family history of Diabetes and/or High Blood Pressure With an annual Optomap, our doctors can track your eye health for concerns, comparison, and treatments. Because Medical and Vision insurances do not pay for routine photos, there is a $39.00 fee for this procedure. The Optomap eliminates the need to be dilated with drops, in most cases. (Please advise staff if you have history of epilepsy.) Visual field testing can assist in early detection of diseases along the optic nerve pathway. Glaucoma and neurological conditions that cause damage to central and peripheral vision can be detected early in the disease process with this technology. We are committed to the prevention of eye diseases and want to stress that early detection is the key to long term health. ______ I ELECT to have an Optomap Digital scan of my retina. Fee: $39.00+Tax (Not covered by insurance) ______ I ELECT to do the package which consists of both the Optomap retinal scan and Visual Field. Fee: $49.00+Tax (Not covered by insurance) ______ I DECLINE the Optomap and choose to be dilated today. I understand that my vision will be slightly blurry and light sensitive for 3-4 hours after dilation. No fee. Covered by insurance. ______ I DECLINE BOTH the Optomap and dilation. I understand that the potential for partial or total loss of vision may exist due to undetected eye disease. I therefore release Dr. Tachau and associates from any liability resulting from failure to diagnose or treat any eye condition due to the lack of diagnostic information, which could have been obtained by performing these tests. Signature: __________________________________________________________ Date: _________________