Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
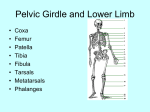
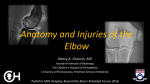
Medial Epicondylitis Medial Epicondylitis is often referred to as “golfer’s elbow” or “baseball elbow”. Persons with medial epicondylitis often have pain over the inside of the elbow (medial epicondyle) and have pain with resisted wrist bending or stretching. Anatomy: The elbow consists of a junction between two bones: the humerus, which extends from the shoulder to the elbow; and the ulna, which meets the humerus at the elbow joint and extends to the wrist. The term “medial epicondyle refers to the large bony area located on the inside of the end of the humerus. Muscles which flex(bend) the wrist originate from the medial epicondyle and cross both the wrist and elbow joints. These muscles are the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and the flexor digitorum superficialis muscles. When these muscles contract, they become shorter, and the tendons of these muscles become taut. The pronator teres muscle, which turns the palm of the hand down, also inserts on the medial epicondyle. Cause: Medial epicondylitis is usually found in people who repetitively overuse or strain these muscles. Therefore, forceful wrist bending or pronation such as in pitching a baseball, throwing a javelin, carrying a heavy suitcase, serving in tennis, gardening, playing a musical instrument, or performing carpentry activities such as screwing or hammering may cause inflammation and/or damage of the tendons which attach to the medial epicondyle. If one continues to stress the muscles, which attach to the medial epicondyle, the tendons may be pulled from the bone and cause an avulsion fracture. An avulsion fracture occurs when the tendon and a small piece of bone attached to the tendon is broken away from the medial epicondyle. Stages: There are two stages of medial epicondylitis: Acute: During this stage, one may take an anti-inflammatory agent. Resting the wrist and elbow and applying ice to the inflamed areas is recommended. In physical therapy, electrical stimulation, pulsed ultrasound, and the application of a splint may be used. Chronic: During this stage, heat is applied to the area before beginning gentle stretches and isometric exercises for the wrist flexors and pronators. Ultrasound, phonophoresis, iontophoresis, and soft tissue massage are used to decrease swelling and pain. Ice is also applied to decrease swelling and pain. In time, one with medial epicondylitis will begin active and resisted wrist flexion and pronation exercises. Prevention: To prevent the reoccurrence of medial epicondylitis, one must continue to perform exercises to increase the strength, power, endurance, and flexibility of the wrist flexors and pronators. Also, it is necessary to modify activities of daily living to prevent unnecessary stress upon these muscles. Modification of existing equipment or activities performed with wrist flexors will help prevent future medial epicondylitis discomfort. Norman 2475 Boardwalk Norman, OK 73069 PH (405) 447-1991 Newcastle 2340 N.W. 32nd Newcastle, OK 73065 PH (405) 392-3322 www.TherapyInMotion.net Purcell 2132 N. Green Ave Purcell, OK 73080 PH (405) 527-1500