Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Germ theory of disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Molecular mimicry wikipedia , lookup
Behçet's disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Sjögren syndrome wikipedia , lookup
DNA vaccination wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Globalization and disease wikipedia , lookup
Marburg virus disease wikipedia , lookup
Herpes simplex wikipedia , lookup
Henipavirus wikipedia , lookup
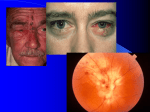
Viral eye infections…. and antivirals to treat them Herpes simplex virus type 1 Human herpesvirus, infects 40-70% -Primary infection neuronal latency and persistence for life sproradic or induced reactivation Recurrence disease Recurrent stromal keratitis -immune mediated- collagen disorganization and scarring -blindness requires corneal transplant - defined by the genetics of virus and host - Many shed very frequently- no disease! epithelial keratitis Stromal keratitis Primary infection Infection of neurons latency reactivation of HSV-1 axonal transport Regulating HSV Lytic/ latent switch -Latency in sensory neurons ( autonomic also?) -viral DNA is episomal and highly chromatin regulated -Only main expression is HSV Latency Associated Transcript -LAT abundantly made at latency -No protein miRNAs? -innate and adaptive cellular Immunity play a role in latency Treating HSV-1 ocular disease Primary infection and Epithelial keratitis Antivirals– ACV or Valtrex- to remove and kill virus Keratitis and stromal disease -disease is immune mediated -goal is to reduce inflammation -STEROIDS -ALWAYS USE AN ANTIVIRAL COVER!!! Varicella zoster virus (VZV) Human herpesvirus, related and like HSV-1 Chickenpoxneuronal latency (decades) zoster (Shingles), pain and PHN Primary VZV infection Chickenpox • Inhaled by aerosol • Infects immune T cells – tonsils/Waldemyers ring – Transfer to T cells in lymph nodes • Reaches skin by T cell viremia systemic spread • T cell Infiltrate skin –virus seeded in dermal skin layers- Perry and Whyte 1998 • 10-21 days- regulated by innate (IFNa/b) until adaptive immunity develops • VZV cleared by adaptive immunity • Problematic in adults- PneumoniaLumpkin E A et al. 2010 Establishment of the VZV latent state • VZV in skininfects sensory nerve axon endings retrograde axon transport • Also VZV in T cells directly infiltrate ganglia neuronal latency • VZV systemic spread - entire neuraxis over body autonomic and sensory ganglia Vaccination Live Attenuated varicella vaccine- OKA • Now mandated in US - 5+ years of age • Live attenuated by passage in cuture • -1200 pfu cell sonicate given in arm x 2 – Virus Infects body, but impaired in skin growth long term protection from disease (not VZV infection) • 86-95% effective in children • Induces Herd Immunity- reduce spread in those not protected Shift the incidence of chicken pox to older ages (adults)? If no varicella-will this reduce boosting of immunity throughout life from subclinical exposure? • Lead to earlier zoster? Herpes zoster -in 1/3 of adult lifetimes -one sided --1 in 20 get zoster on head Termed HZO if VZV reactivates from 5th cranial nerve Disease limited to a dermatome What’s different from HSV-1 reactivation? - frequency and age - ganglionic (zosteriform) spread - ganglionitis and damage - one neuron involved (HSV) versus many (VZV) Zoster- Risk Factors Triggers of zoster? Age – – 84% of cases occur after 60 – more in women Cellular immune status – – – – AIDS Radiation Therapy Cancer (esp. lymphoma) medical immunosupression therapies BMT & Transplants (30-55% in a year!) CD4 appear more important than CD8 in preventing zoster Is there subclinical reactivation during life? Harpaz R et al 2008 Examples of ocular zoster VZV Can infect every ocular tissue to cause: Punctate epithelial keratitis (PEK) Dendritic keratitis – -w/o terminal bulbi Stromal keratitis/inflammation – -Harder to treat than HSV-1 Neurotrophic keratitis – -Total loss of corneal sensation – -iatrogenic ulceration Rarer Findings Uveitis, retinitis, Acute retinal necrosis. Neurotrophic Keratopathy The “diabetic foot” of the eye • ~ 8% of HZO patients develop total loss of corneal sensation ~ 3% of HZO patients develop neurotrophic ulceration Iatrogenic insults are the main reason that neurotrophic corneas get into trouble. VZV and Pain • 1 million people a year in the US • 90% will seek prescribed medication for pain • 30% will develop debilitating chronic pain Post Herpetic Neuralgia (PHN) • Very difficult to treat (uses • Many PHN patients get no benefits from any form of treatment Why is there pain? Ganglionitis Ganglionic necrosis Neuronal connective plasticity and reorganization Demyelyination Cell-Neuron Fusion-cytoplasmic mixing Other ocular/ neurological complications of VZV • Most are rare and mis-diagnosed • Persistent VZV in CNS vasculature or CNS/brain leads to …. • • • • • • Cognitive deficits Stroke Headaches Migraines? seizures Vaccination to prevent zoster – Zostervax- same as varicella vaccine- 14X more virus – VZV immune people get it. – Recommended > 50 yrs, may eventually need two doses – Is the only human herpesvirus vaccine so far – Partial efficacy - not everyone is protected – 51% drop in zoster incidence – 68% fall in “burden of illness” (including PHN) Adenovirus follicular conjunctivitis vs others-differential diagnosis Adenoviral Infections • non-enveloped virus, • 34Kbp DS-DNA, many viral proteins • At least 57+ identified Serotypes • Three major ocular diseases • Epidemic Keratoconjunctivitis ( 8, 19 and 37+ several new serotypes and interrecombinant strains) • Pharyngoconjunctival fever (3,4, & 7) Epidemic Kerato-conjunctivitis transferred by hands, instruments, solutions. Adenoviruses survive >35 days on dry surface Epidemics arise from ophthalmologists offices. Patients remain infectious for 14 days after onset Usually One eye, then other (milder) Lasts 7 days -2 weeks Source of new isolates- Japan/Asia - Japan-EKC is a reportable disease - Hawaii west coast -mixing ground Clinical Symptoms Foreign Body Sensation Tearing Photophobia Sore Throat Breathing Problems Conjuntivitis NO ANTIVIRAL – YET – -Correct timely diagnosis an issue After virus…... -Subepithelial infiltrates (immune mediated) -last weeks to months - treat with steroids - requires slow withdrawal Adenovirus EKC management Ebola Virus EBV in Ocular Fluid during convalescence Varkey, JB et al NEJM, 2014 Zika virus Human RNA alphavirus transmitted by mosquitos Also transmitted in utero and by sexual contact 80% have no symptoms Fever rash, arthritis and conjunctivitis are common No known antiviral or vaccine – yet Of most concern is ocular development in newborns with microcephaly Ocular complications in newborns • Retinal bleeding (Hemorrhagic retinopathy) • Abnormal blood vessel development (missing vessels) • Torpedo maculopathy (topedo shaped lessions in macula A model of Zika and eye disease? Miner et al., 2016, Cell Reports 16, 3208–3218 September 20, 2016 Highlights a. ZIKV infects several different regions of the eye, including the Retina. ZIKV infected the iris, cornea, retina, and optic nerve and caused conjunctivitis, panuveitis, and neuroretinitis in mice. b ZIKV RNA can be detected in tear fluid c Eye and brain infection in adult mice by ZIKV occurs independently of the AXL receptor d ZIKV infection results in apoptosis of neurons of the visual processing pathway CMV and retinitis • 80% are seropositive • Virus is endemicearly childhood • Usually asymptomatic • Retinitis Rare outside of HIV/AIDS -A major factor in “will to live” Of AIDS patients Signs Photophobia Eye Pain/redness Floaters Vision loss Usually initiates monocular Other Viruses causing conjunctivitis or Eye Disease CM and EBV herpesviruses affecting most people – may cause conjuntivitis and ,rarely, corneal keratitis Entero/coxsaccivirus- Hemorrhagic conjunctivitis -begins as eye pain, then red, watery eyes with swelling, - light sensitivity, and blurred vision. HIV (and everything resulting from it) Newcastle disease virus Vaccinia Mollocsum contageosum (lid lesions) Papilloma (lid lesions) Measles (Conujuntivitis) Important Ophthalmic antivirals Triflorothymidine (viroptic) HSV-1>> VZV Acyclovir and valacyclovir HSV-1 and VZV Ganciclovir and valganciclovir CMV retinitis, Adeno, Foscarnet (phosphonoformate) CMV (GCVr)> HSV,VZV Cidofovir CMV (GCVr) HAART HIV/AIDs Trifluridine (viroptic) Analog of deoxyuridine nucleoside Incorporated into DNA CF3 blocks base pairing in DNA Has higher affinity for viral DNA pol over cell pol Used topically only- toxic systemically Acyclovir, gancyclovir and derivatives Acyclovir (FDA licensed in 1981) Use Herpes simplex virus Varicella Zoster virus human cytomegalovirus 0.1-3 ug/ml 5-20 60-200 (not deemed “clinically effective”) Safe in Long term Prophylaxis treatments Prodrug mechanismonly active in virus infected cells Virtually non toxic in uninfected cell 100 x more active in HSV—1 infected cell. Once activated, has higher affinity (50x) for HSV DNA polymerase over cellular DNA polymerase. ACV Mechanism of Action –HSV VZV Thymidine (nucleoside) Kinase activates it –ACV TP binds Viral DNA polymerase >>>>> cell pol –Incorporated into DNA - acts as DNA chain terminator ACV - Resistance Readily arises in culture – Defect /loss of viral TK – Mutation of DNA polymerase- alters ACV affinity rarely occurs in vivo- why? – – – – – Latency in neurons TK needed for HSV reactivation TK- viruses don’t reactivate ACVR arise In AIDS patients with long treatments Have Pol mutations: or Low persistent viral replication: or Have minimal TK levels sufficient to enable reactivation from latency – Not sufficient to activate/ phoshorylate ACV Oral forms of Acyclovir Liver Acyclovir ACV Valacyclovir “Valtrex” alone is degraded by the stomach Valine Ester derivative has high oral- bioavailability –e.g. 63-72% absorption vs 15% for ACV Is de-esterified by liver on first pass ACV Allows reduced dosing and taking by mouth GMP O Ph O N N N Gancyclovir N N O To 5’ end N N N O N N O O O to 3’ end Gancyclovir and Valgancyclovir drugs to combat HCMV disease Ganciclovir (Cytovene) used for hCMV also used for stubborn VZV and HSV works much better than ACV for CMV disease – retinitis and systemic disease in transplant patients BUT GCV Requires IV dosing but val-GCV (ester form) by mouth – GCV is More toxic than ACV- Why? GCV-PPP also inhibits host cell polymerasemuch less selective – GCV Does not cross retinal/brain barriers well Often use ocular implants for retinitis GCV increases AZT toxicity- bad for HIV patients GCV-a Mechanism of action GCV DNA chain terminator O –CMV has no TK gene –CMV uses a protein kinase (UL97) to phosphorylate GCV (and ACV) N N GCV Resistance O • Arises due to long treatment for CMV diseases (upto 10% In Retinitis and organ transplants) N N O O •Rare- mutations in UL97 protein kinase •( UL97 is needed for hCMV to efficiently assemble) •Mutations in DNA polymerase that alter affinity • High GCV-resistant CMV have both genes altered N Foscarnet (phosphonoformate, PFA) • Mechanism of action: – – – – – All polymerases need P-P as cofactor PFA analog of pyrophosphate (P-P) binds to DNA polymerase PFA blocks P-P binding resistance – altered DNA polymerase P-P O OH OH P P OH OH O • Efficacy/toxicity – active on nucleoside resistant viruses • Acts at different site to GCV/ACV – Toxic in bone, kidney, neuronal deposits • Uses: – CMV retinitis and GCVr CMV in transplants – rare use on HSV and VZV ARN – Rare use on systemic HSV and VZV O OH OH P OH PFA CH O Nucleoside phosphonates •Cidofovir •Licensed for CMV retinitis •Analogs of dNMPs – no initial P step needed • CDV has long intracellular half life •Has activity to many viral DNA polymerases •Works against : many adenoviruses, poxviruses, -(used if smallpox resurrects?) herpesviruses , polyomaviruses, HBV? Could be the universal antiviral drug in not so toxic Lipid Conjugate Technology Exploits Natural Phospholipid Pathways CMX001 Lysolecithin Polar head Non-polar tail Cidofovir Lipid conjugation enhances absorption and distribution CMX001 Cidofovir Broadly active against dsDNA Orders of magnitude more potent than CDV; broadly active Initially being developed for adenovirus, CMV and smallpox Requires intravenous infusion Orally available Black box warning for renal No evidence of nephrotoxicity or myelotoxicity viruses Approved for treatment of CMV retinitis in patients with AIDS impairment and neutropenia