Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Taura syndrome wikipedia , lookup
Hepatitis C wikipedia , lookup
Neonatal infection wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Orthohantavirus wikipedia , lookup
Canine parvovirus wikipedia , lookup
Henipavirus wikipedia , lookup
Hepatitis B wikipedia , lookup
Marburg virus disease wikipedia , lookup
Canine distemper wikipedia , lookup
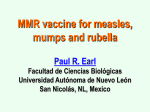
Mumps,Measles,Rubella DR;RIADH ABDULATIF ALOBAIDY differential diagnosis of Fever and rash syndrome 1-Maculopapuler;measles,roseola,fifth disease, EB virus, scarlet fever, rheumatic fever, ricketsiae. 2-Diffuse erythroderma; scarlet fever, toxic shock syndrome(staph. aureus); Scarlentiform rash. 3-Urticarial; mycoplasma, EB virus 4- vesiculobullous; Herpes simplex, varicella, staphyllococal bullous impetigo, staphyliococcal scalded skin syndrome 5-petechial -purpuric Viruses; congenital rubella syndrome, cytomegalovirus. Bacteria; sepsis; meningococcal, pneumococcal, H. influenza, Mumps is an acute self-limited infection, now unusual in developed countries because of widespread use of vaccination. It is characterized by fever, bilateral or unilateral parotid swelling and tenderness, and the frequent occurrence of meningoencephalitis and orchitis. Although no longer common in countries with extensive vaccination programs, mumps remains endemic transmission Mumps is spread from person to person by respiratory droplets. Virus appears in the saliva from up to 7 days before to as long as 7 days after onset of parotid swelling. The period of maximum infectiousness is 1-2 days before to 5 days after onset of parotid swelling CLINICAL FEATURES The incubation period is 16-18 days resulting in clinical presentation ranging from asymptomatic to the typical illness associated with parotitis. The typical patient presents with a prodrome 1-2 days and consisting of fever, headache, and vomiting. Parotitis then appears and may be unilateral ,then becomes bilateral in about 70% of cases .The parotid gland is tender, and may be accompanied by ear pain on the ipsilateral side. Sour foods or liquids may enhance pain in the parotid. As swelling progresses, the angle of the jaw filled and earlobule is pushed outward. The opening of Stensen duct may be red and edematous. The parotid swelling peaks in approximately 3 days, then gradually subsides over 7 days. Submandibular salivary glands may also be involved or may be enlarged without parotid swelling. Edema over the sternum due to lymphatic obstruction may also occur Mumps and normal Differential diagnosis Purulent parotitis, is usually caused by Staphylococcus aureus, unilateral, extremely tender, and is associated with an elevated white blood cell count, and may involve purulent drainage from Stensen duct. Submandibular or anterior cervical adenitis due to a variety of pathogens may also be confused with parotitis. complications The most common complications of mumps are meningitis, with or without encephalitis, and orchitis. Uncommon complications include deafness, facial palsy, pancreatitis, and thrombocytopenia. Maternal infection with mumps during the 1st trimester of pregnancy results in increased fetal wastage. No fetal malformations have been associated with intrauterine mumps infection. Meningoencephalitis Symptomatic m.e. occurs in only10-30% of mumps cases, but CSF pleocytosis has been found in 40-60% of patients as subclinical more than apparent meningitis. The meningoencephalitis is usually benign, may occur before, along with, or following the parotitis Orchitis Involvement in young boys is rare, but in adolescent and after puberty, orchitis occurs in 30-40% of male cases. Atrophy of the testes may occur, but sterility is rare even with bilateral involvement. prevention Antibody develops in 95% of children after 1 vaccine dose.. As a live- vaccine, MMR should not be administered to pregnant women or to immunodeficient child. Measles Measles is highly contagious disease. Owing to widespread vaccination, transmission is limited . Measles virus is a single-stranded, lipidenveloped RNA virus in the family Paramyxoviridae and genus Morbillivirus Transmission The portal of entry of measles virus is through the respiratory tract or conjunctivae following contact with aerosol droplets in which the virus is suspended. Patients are infectious from 3 days before -to 4-6 days after the onset of rash Clinical manifestations Measles is a serious infection characterized by high fever,cough,coryza, conjunctivitis ,enanthem ,and a prominent exanthem (the rash). ` After an incubation period of 8-12 days, the prodromal phase (2-4) days begins with a mild fever followed by conjunctivitis with photophobia, coryza, a prominent cough, and increasing fever. Koplik spots represent the enanthem and are the pathognomonic sign of measles, appearing 12-24 hours before the onset of the rash and it last for 1-2 days after rash appearence. They first appear as sandy white spots on minute red lesions in the inner aspects of the cheeks at the level of the lower premolars... Koplik spots have been reported in 5070% of measles cases. KOPLIK SPOTS MEEASLES Clinical features con. Symptoms increase in intensity for 2-4 days until the 1st day of the rash. The rash begins on the forehead (around and before the hairline), and behind the ears as a red maculopapular eruption. It then spreads to the face and upper neck and downward to the trunk and extremities,and reaching the palms and soles in up to 50% of cases.. The rash last 5-6 days, then fades over about 7 days in the same manner as it evolved, often leaving a fine desquamation of skin. Of the major symptoms of measles, the cough lasts the longest, often up to 10 days. In more severe cases, generalized lymphadenopathy may be present, with cervical and occipital lymph nodes enlargement. Diagnosis Mainly clinical but more convenient confirming serological test can be done by high antibody IgM level . Blood and urine samples for viral culture is the most commonly WHO protocol for detection of the illness. Differential diagnosis ; include other fever and rash illnesses like rubella , roseola, erythema infectiosum, adenovirus, EB virus and enteroviruses. Scarlet fever and kawasaki synderome. Drug eruption Complications Pneumonia is the most common cause of death in measles. It may manifest as giant cell pneumonia caused directly by the viral infection or as superimposed bacterial infection. Croup, tracheitis, and bronchiolitis are common complications in infants and toddler. Acute otitis media and pneumonia are the most common complication of measles, vomiting and diarrhea. Encephalitis 1;3000 of cases by direct viral infection or postinfectious and may be fatal. Rarely Fatal Hemorrhagic measeles (black measles) leading to hemorrhagic skin lesions. Subacute sclerosing panenecephalitis is rare . It is slow virus infection infect the CNS developed in 7-10 years after measles and it is fatal. treatment Mainly supportive as antipyritics and rehydration and respiratory suppport .. Vitamine A defeciency is common in developing countries and is associated with high mortality in measles so jt is recommended to give it to the patients. Single dose of 200,000 IU orally for children ≥1 yr of age, 100,000 IU for children 6 mo–1 yr of age, and 50,000 IU for infants <6 mo of age . prevention Shedding measles virus from 7 days after exposure to 4-6 days after the onset of rash. Exposure of susceptible individuals to patients with measles should be avoided during this period . A 2-dose schedule (with MMR) is recommended for full immunity. The first dose is recommended at 12-15 mo of age; the 2nd is recommended at 4-6 yr of age. For immune deficient if exposed to a case immune globulin I M should be given. RUBELLA Rubella (German measles or 3-day measles) is a mild, often exanthematous disease of infants and children, but is more severe and associated with more complications in adults. Its major clinical significance is transplacental infection and fetal damage as part of the congenital rubella syndrome (CRS Clinical Manifestations Postnatal infection rubella is a mild disease . Following an incubation period of 14-21 days, a prodrome consisting of low-grade fever, sore throat, red eyes, headache, malaise, anorexia, and lymphadenopathy begins. Suboccipital, postauricular, and anterior cervical lymph nodes are most prominent. In children, the 1st manifestation of rubella is usually the rash, which is variable and not distinctive. It begins on the face and neck as small, irregular pink macules that coalesce, and it spreads to involve the trunk and extrimities .The duration of the rash is generally 3 days, and it usually resolves without desquamation Congenital rubella syndrome Deafness 67% Ocular 71% Cataracts 29 % Retinopathy 39% Heart disease 48% Patent ductus arteriosus 78 % Right pulmonary artery stenosis 70% Left pulmonary artery stenosis 56 % Valvular pulmonic stenosis 40 % Low birthweight 60% Psychomotor retardation 45% Neonatal purpura 23%.Death %35 MMR vaccine Vaccine should not be administered during pregnancy.. Studies of >200 women who had been inadvertently immunized with rubella vaccine during pregnancy showed that none of their offspring developed CRS. Therefore, interruption of pregnancy is probably not warranted