Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
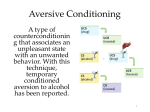
Chapter 17 notes – Therapies ‘15 Science’s achievements vs. psych…; reformers Pinel, Dix, (Freud) 1. Psychological therapies: psychotherapy, eclectic approach / psychotherapy integration Psychoanalysis: focus / aims, methods (add resistance, transference, insight to chapter 15 techniques), pros, cons -psychodynamic, interpersonal Humanistic: focuses, client-centered therapy, nondirective, genuineness, acceptance, empathy, active listening – paraphrase, invite clarification, reflect feelings Behavior therapies: focus, Classical conditioning: counterconditioning, systematic desensitization (Mary Cover Jones), Wolpe – exposure therapies, hierarchy, progressive relaxation, virtual reality exposure therapy, implosion / flooding; aversive conditioning Operant conditioning: token economy, behavior modification Cognitive therapies: the cognitive revolution!!! for depression; Beck, Ellis – cognitive errors: (ie. catastrophizing, awfulizing, musterbation, fortune-telling error, magnification, minimization), Rational Emotive Therapy (RET) --integrated: stress inoculation training, cognitive-behavioral therapy Group and Family therapies (all except psychoanalysis): pros and cons, Alcoholics Anonymous Evaluating psychotherapies: clients perceptions, clinicians’ perceptions – vs. self-justification / regression to the mean / placebo effect… -Outcome research: Eysenck challenge vs. Smith , meta-analysis, newer studies (figure 17.4, pg 703) -relative effectiveness of each -evaluating alternative therapies: eye movement desensitization and reprocessing (EMDR), light exposure therapy Psychotherapy commonalities: hope, new perspective, empathy / trust / concern / a relationship, Culture and values: Ellis vs. Bergen Consumer’s guide: psychiatrists, clinical psychologists, clinical / psychiatric social workers, counselors 2. Biomedical therapies -- Drug therapies / psychopharmacology, double-blind technique, DEINSTITUTIONALIZATION Antipsychotic drugs: Thorazine (chlorpromazine) – D2, Clozaril (clozapine) and Risperdal, Zyprexa – D1; effects, side effects, tardive dyskinesia Antianxiety: Valium, Xanax, Atavan; effects, side effects Antidepressants: Prozac! (fluoxetine) vs. MAOIs, tricyclics; SSRIs: Prozac, Paxil (some for OCD), Zoloft, Celexa, Lexapro (Wellbutrin also affects dopamine and norepinephrine), effects, popularity, placebos, exercise -bipolar: some of these and lithium Electroconvulsive therapy (ECT), repetitive transcranial magnetic stimulation (rTMS): Psychosurgery – Egas Moniz – lobotomy cingulotomy; largely abandoned… Health psychology / Preventing: “upstream work” Chapter 17 notes – Therapies ‘15 Science’s achievements vs. psych…; reformers Pinel, Dix, (Freud) 1. Psychological therapies: psychotherapy, eclectic approach / psychotherapy integration Psychoanalysis: focus / aims, methods (add resistance, transference, insight to chapter 15 techniques), pros, cons -psychodynamic, interpersonal Humanistic: focuses, client-centered therapy, nondirective, genuineness, acceptance, empathy, active listening – paraphrase, invite clarification, reflect feelings Behavior therapies: focus, Classical conditioning: counterconditioning, systematic desensitization (Mary Cover Jones), Wolpe – exposure therapies, hierarchy, progressive relaxation, virtual reality exposure therapy, implosion / flooding; aversive conditioning Operant conditioning: token economy, behavior modification Cognitive therapies: the cognitive revolution!!! for depression; Beck, Ellis – cognitive errors: (ie. catastrophizing, awfulizing, musterbation, fortune-telling error, magnification, minimization), Rational Emotive Therapy (RET) --integrated: stress inoculation training, cognitive-behavioral therapy Group and Family therapies (all except psychoanalysis): pros and cons, Alcoholics Anonymous Evaluating psychotherapies: clients perceptions, clinicians’ perceptions – vs. self-justification / regression to the mean / placebo effect… -Outcome research: Eysenck challenge vs. Smith , meta-analysis, newer studies (figure 17.4, pg 703) -relative effectiveness of each -evaluating alternative therapies: eye movement desensitization and reprocessing (EMDR), light exposure therapy Psychotherapy commonalities: hope, new perspective, empathy / trust / concern / a relationship, Culture and values: Ellis vs. Bergen Consumer’s guide: psychiatrists, clinical psychologists, clinical / psychiatric social workers, counselors 2. Biomedical therapies -- Drug therapies / psychopharmacology, double-blind technique, DEINSTITUTIONALIZATION Antipsychotic drugs: Thorazine (chlorpromazine) – D2, Clozaril (clozapine) and Risperdal, Zyprexa – D1; effects, side effects, tardive dyskinesia Antianxiety: Valium, Xanax, Atavan; effects, side effects Antidepressants: Prozac! (fluoxetine) vs. MAOIs, tricyclics; SSRIs: Prozac, Paxil (some for OCD), Zoloft, Celexa, Lexapro (Wellbutrin also affects dopamine and norepinephrine), effects, popularity, placebos, exercise -bipolar: some of these and lithium Electroconvulsive therapy (ECT), repetitive transcranial magnetic stimulation (rTMS): Psychosurgery – Egas Moniz – lobotomy cingulotomy; largely abandoned… Health psychology / Preventing: “upstream work” Chapter 17: Therapy version 1 Philippe Pinel (France) and Dorothea Dix (US) advocated constructing mental hospitals to offer more humane methods of treatment. Psychological Therapies – employ structured interactions (usually verbal) between a trained professional and a client with a problem. Biomedical Therapies - act directly on the patient’s nervous system. The Psychological Therapies - Psychotherapy – an emotionally charged, confiding interaction between a trained therapist and someone who suffers from psychological difficulties. - Eclectic Approach – an approach to psychotherapy that, depending on the client’s problems, uses techniques from various forms of therapy. - Psychotherapy integration – aims to combine techniques or methods into a single, coherent system. Psychoanalysis o Sigmund Freud’s therapeutic technique. o Freud believed the patient’s free associations, resistances, dreams, and transferences—and the therapist’s interpretations of them—released previously repressed feelings, allowing the patient to gain self-insight. Aims Assumes that many psychological problems are fueled by childhood’s residue of repressed impulses and conflicts Aim to bring the repressed feelings into conscious awareness where the patient can deal with them. With insight, the patient works through the buried feelings. To help patients release the energy they had previously devoted to id-ego-superego conflicts. Methods Free association – relax, focus attention on your own thoughts and feelings; start with a childhood memory, dream, experience and say whatever is on your mind from moment to moment. Resistance – blocks in the flow of your free associations; hint that anxiety lurks and that you are repressing sensitive material. Interpretations – the analyst’s noting supposed dream meanings, resistances, and other significant behaviors in order to promote insight; through this, the patient may discover what he is avoiding and what his resistances mean and how they fit with other pieces of your psychological puzzle. Latent content – the underlying meaning of a dream Transference – the patient’s transfer to the analyst of emotions linked with other relationships; may be caused due to the strong bond of sharing your deepest thoughts with your psychoanalyst. Based on assumption that repressed memories exist; not seeing the interpretations of your analyst may be seen as more resistance. Difficult to disprove or prove interpretations. Psychodynamic Therapy Try to understand a patient’s current symptoms by exploring childhood experiences and probing for supposed repressed, emotion-laden information, seeking to help the person gain insight into the unconscious roots of problems and work through newly resurrected feelings. Interpersonal psychotherapy – a brief alternative psychodynamic therapy that has been found effective with depressed patients; aims to help people gain insight into the roots of their difficulties; rather than focusing on undoing past hurts and offering interpretations, this focuses on current relationships and assists in improving relationship skills. Humanistic Therapies o Emphasizes people’s inherent potential for self-fulfillment o Aims to boost self-fulfillment by helping people grow in self-awareness and self-acceptance o Focuses on the present and future more than the past, the conscious rather than the unconscious thoughts, taking immediate responsibility for one’s feelings and actions, and promoting growth. Client-Centered Therapy – by Carl Rogers; the therapist uses techniques such as active listening within a genuine, accepting, and empathic environment to facilitate clients’ growth. o Nondirective therapy – refraining from directing the client toward certain insights. o Rogers encouraged therapists to exhibit genuineness, acceptance, and empathy; insist on making clients feel unconditionally accepted so that they deepen their self-understanding and self-acceptance. o Active Listening – empathic listening in which the listener echoes, restates, and clarifies; counselor interrupts only to restate and confirm the client’s feelings, tot accept what the client is expressing, or to seek clarification. o Unconditional Positive Regard – where the client feels accepted and understood in a nonjudgmental, grace-filled environment. Behavior Therapies o doubt the healing power of self-awareness and assume that behaviors are the problems. o Applies learning principles to eliminate the unwanted behavior o View maladaptive symptoms as learned behaviors, which they try to replace with constructive behaviors Classical Conditioning Techniques Counterconditioning – a behavior therapy procedure that conditions new responses to stimuli that trigger unwanted behaviors For example, to stop bed-wetting, the child sleeps on a liquid-sensitive pad connected to an alarm. Moisture on the pad triggers the alarm, waking the child. The association of urinary relaxation with waking up stops the bed-wetting and improves self-image. Systematic Desensitization – associates a pleasant relaxed state with gradually increasing anxiety-triggering stimuli; commonly used to treat phobias. For example, Peter is scared of rabbits. He eats lunch with a rabbit in a cage. The following days, he continues to eat lunch, but the rabbit moves closer every day, and soon ends up on his lap, and his fear is replaced with relaxation. Exposure Therapies – behavioral techniques, such as systematic desensitization, that treat anxieties by exposing people to the things they fear and avoid. Progressive Relaxation – therapist trains you to relax one muscle group after another, until you achieve a drowsy state of complete relaxation and comfort, and then imagine a mildly anxietyarousing situation. If this causes anxiety, you raise your finger and are told to return to relaxation, while the scene is repeatedly paired with relaxation, and continue until there is no trace of anxiety. Virtual Reality Exposure Therapy – wearing a head-mounted display unit that projects a 3D virtual world, the client is immersed into a lifelike series of scenes. Aversive Conditioning – a type of counterconditioning that associates an unpleasant state with an unwanted behavior. For example, to treat alcoholism, the alcoholic drink is mixed with a nausea-causing drug. The drinker feels nauseated and associates alcohol with nausea, stopping the desire to drink. This may not work because the patient knows that he/she can drink outside the therapist’s office without fear of nausea. Operant Conditioning This enables therapists to reinforce desired behaviors and to withhold reinforcement for, or to punish, undesired behaviors because voluntary behaviors are strongly influenced by their consequences. The combination of positive reinforcing of desired behaviors and ignoring or punishing aggressive and self-abusive behaviors worked wonders. Token Economy – awards desired behaviors. A patient exchanges a token of some sort, earned for exhibiting the desired behavior, for various privileges or treats. Two Problems: 1) After the reinforcements stop, they may become so dependent on extrinsic rewards that the appropriate behaviors quickly disappear. 2) It is not right for one human to have total control over another’s behavior by use of reinforcers. Cognitive Therapies o Cognitive Therapies – therapy that teaches people new, more adaptive ways of thinking and acting; based on the assumption that thoughts intervene between events and our emotional reactions o Influenced how therapists treat these less clearly defined psychological problems and has profoundly changed psychology during the last four decades. o o Try in various ways to teach people new, more constructive ways of thinking. Cognitive Therapy for Depression Beck analyzed the dreams of patients with depression and found recurring negative themes of loss, rejection, and abandonment that extended into their waking thoughts. Seek to reverse clients’ catastrophizing beliefs about themselves, their situations, and their futures Attempt to convince depressed people to take off the dark glasses through which they view life, and their technique is a gentle questioning that aims to help people discover their irrationalities Often combine the reversal of self-defeating thinking with efforts to modify behavior (CognitiveBehavior Therapy). Seeks to make people aware of their irrational negative thinking, to replace it with new ways of thinking, and to practice the more positive approach in everyday settings. Stress Inoculation Thinking – restructuring thinking in stressful situations by saying more positive things to oneself. Group and Family Therapies o Its social context allows people both to discover that others have problems similar to their own and to try out new ways of behaving. o It can help to receive feedback and be a relief to find that you are not alone, that other people share your problems and your troublesome feelings. o Most support groups focus on stigmatized, embarrassing, hard-to-discuss illnesses. o Family therapy – views an individual’s unwanted behaviors as influenced by or directed at other family members; attempts to guide family members toward positive relationships and improved communication. o Family therapists work with family groups to heal relationships and to mobilize family resources and aim to help family members discover the role they play within their family’s social system. Evaluating Psychotherapies - most psychotherapy now is done by clinical and counseling psychologists - Much of it is done through community mental health programs, which provide outpatient therapy, crisis phone lines, and halfway houses for those making the transition from hospitalization to independent living. Is Psychotherapy Effective? Clients’ Perceptions ¾ clients reported themselves satisfied and ½ reported themselves very satisfied; those who reported feeling fair or very poor before therapy now, 9/10 now were feeling very good or at least so-so. May not persuade psychotherapy’s skeptics because 1) People often enter therapy in crisis and may attribute their otherwise normal ebb and flow of events to the aid of therapy. 2) Clients may need to believe the therapy was worth the effort. Self-justification is a powerful human motive. 3) Clients generally like their therapists and speak kindly of them. Even if the problem remains, they work hard to find something positive to say. Testimonials can be misleading, by use of the self-serving bias. Clinicians’ Perceptions Therapists are aware of failures, but mostly of other therapists, whose clients have come to them. The client’s continuous problem and switching of therapists may cause a “success story” in each therapist’s files. Because people enter therapy when they are extremely unhappy, most therapists testify to therapy’s success—regardless of the treatment. Outcome Research meta-analysis – a procedure for statistically combining the results of many different research studies. Those not undergoing therapy often improve, but those undergoing therapy are more likely to improve. The Relative Effectiveness of Different Therapies o Depression: cognitive therapy, interpersonal therapy, and behavior therapy o Anxiety: cognitive therapy, exposure therapy, and stress inoculation training o Bulimia: cognitive-behavior therapy o Bed-Wetting: behavior modification Evaluating Alternative Therapies Therapeutic Touch practitioners move their hands a few inches from a patient’s body, “pushing energy fields into balance.”; has been said to heal headaches, burns, cancer, etc. Argued by skeptics and their beliefs of its placebo effect. Emily Rosa schemed an experiment with a screen to block the view of the participant and see if he/she knew which hand Emily was placing her hand above. They averaged 47% correct, disproving therapeutic touch. Eye Movement Desensitization and Reprocessing (EMDR) while imagining traumatic scenes, Shapiro triggered eye movements by waving her finger in front of their eyes. All marked reductions in distress after just one therapeutic session. Probably efficacious for the treatment of nonmilitary post-traumatic stress disorder; applied to other anxiety disorders and those with pain, grief, rage, guilt, paranoid schizophrenia, etc. The therapeutic part of EMDR is the combination of exposure therapy and a robust placebo effect. Light Exposure Therapy seasonal affective disorder, which is oversleeping, gaining weight, and feeling lethargic during the dark mornings and overcast days of winter used to treat SAD; to counteract this, patients are given intense light for a timed daily dose, which tweaks the circadian clock. Using 90 minutes of bright light for four weeks, 61% of users greatly improved. Commonalities Among Psychotherapies o compassion, sensitivity, and empathy o hope for demoralized people, a new perspective on oneself and the world, and an empathic, trusting, caring relationship. Hope For Demoralized People Therapy offers the expectation that, with commitment from the patient, things can and will be better. Promotes improved morale, new feelings of self-efficacy, and diminished symptoms. Each therapy may harness the client’s own healing powers. A New Perspective Therapy can offer new experiences that help people change their behaviors and views of themselves This helps them approach life with a new attitude An Empathic, Trusting, Caring Relationship effective therapists are empathic people who seek to understand another’s experience; whose care and concern the client feels; and whose respectful listening, reassurance, and advice earn the client’s trust and respect. Therapies offer hope through a fresh perspective offered by a caring person. Culture and Values in Psychotherapy o On certain matters of moral and cultural diversity, therapists may differ from one another and from their clients. o Value differences also can become significant because in western civilizations, most therapists reflect their culture’s individualism, while some countries concentrate on being mindful of others’ expectations rather than their own. o Such differences help explain the reluctance of some minority populations to use mental health services. The Biomedical Therapies Drug Therapies o psychopharmacology – the study of effects of drugs on mind and behavior. Antipsychotic Drugs most severe of the drugs. Thorazine – helped with some schizophrenia in the 50’s; used to be used as a tranquilizer; reduces dopamine; major medication with major side effects. Closaril – reduces dopamine and serotonin levels; helps some negative and positive effects of schizophrenia. Antianxieties Physically/psychologically addictive Negative reinforcement Valium, Xanax, Librium, Atavan Used to be the most prescribed drugs Antidepressants Pre-1988: MaOI’/tricyclics; neurogenesis – sprouting new dendrites Prozac used to be very strong when it didn’t need to be Post-1988: SSRI’s (block reabsorption of serotonin) Paxil, Zoloft, Celexa, Lexapro 80% benefit reports; takes up to 6-weeks to feel effects Wellbutrin blocks reabsorption of serotonin, norepinephrine, and dopamine. Electroconvulsive Therapy o ECT – for severely depressed patients in which a brief electric current is sent through the brain of an anesthetized patient o Shocks every neuron in the body o Has the highest rate of success, but used only as the very last resort to curing depression Psychosurgery o surgery that removes or destroys brain tissue in an effort to change behaviors o lobotomy – a now-rare psychosurgical procedure once used to calm uncontrollably emotional or violent patients. The procedure cut the nerves that connect the frontal lobes to the emotion-controlling centers of the inner brain o Lobotomies produced permanently lethargic, immature, and impulsive personalities. Preventing Psychological Disorders - It is better to prevent a problem by reforming a sick situation and by developing people’s coping competencies than to wait for a problem to arise and then treat it. - Preventive mental health is upstream work because it seeks to prevent psychological casualties by identifying and alleviating the conditions that cause them. - There is abundant evidence that poverty, meaningless work, constant criticism, unemployment, racism, and sexism undermine people’s sense of competence, personal control, and self-esteem. - We strive for healthy minds in healthy bodies because stress affects body chemistry; chemical balances can cause depression and schizophrenia, and can threaten our physical health. Chapter 17: Therapy version 2 Transition from brutal to gentle treatment s of psychological disorders Mental health therapies can be classified into two main categories: (1) psychological therapies (2) biomedical therapies Psychological disorders that researchers believe are learned will likely be treated with psychological therapy or psychotherapy[y Psychotherapy-an emotionally charged confiding interaction between a trained therapist and someone who suffers from psychological difficulties Biologically rooted disorders are likely to be treated with biomedical therapy- a prescribed medication or medical procedure that acts directly on patients nervous system Many psychological disorders are also related to social conditions so psychologists want to try to improve the unhealthy environment Eclectic approach- approach to psychotherapy that depending on the client’s problems uses techniques from various forms of therapy The Psychological Therapies Psychoanalysis Sigmund Freud’s techniques survive today especially in psychodynamic therapies Aims Psychoanalytic theory presumes that healthier, less anxious living becomes possible when people release the energy they had previously devoted to id-superego conflicts Methods Freud said hypnosis is unreliable so turned to his idea of free association Blocks in the flow of your free associations indicate resistance- the blocking from consciousness of anxiety laden material Want to make you aware of you resistance and interpret the meaning providing insight into your underlying wishes, feelings, and conflicts Interpretation- the analyst’s noting supposed dream meanings, resistances, and other significant behaviors and events in order to promote insight Freud also believed that your dreams latent content- their underlying but censored meaning- is a clue to the unconscious Transference- the patient’s transfer to the analyst of emotions linked with other relationships Analysts believe that transference exposes feelings that a person has previously defended against giving you a belated chance to work through them with your analyst’s help Psychodynamic Therapy Psychodynamic therapists try to understand a patient’s current symptoms by focusing on themes across important relationships Help patient explore and gain perspective on defended against thoughts and feelings Interpersonal Psychotherapy- is a variation of psychodynamic therapy and has been effective in treating depression; aims to help people gain insight into the roots of their difficulties but its goal is symptom relief in the here and now, not overall personality change Humanistic Therapies Emphasizes people’s inherent potential for self-fulfillment Aim to boost self-fulfillment by helping people grow in self-awareness and self-acceptance Attempt to reduce the conflicts that are impending natural developmental growth Tend to focus on the present and the future more than the past Conscious rather than unconscious thoughts Taking immediate responsibility for one’s feelings and actions rather than uncovering hidden determinants Promoting growth instead of curing illness Client-centered therapy- Carl Rogers- a humanistic therapy developed by Carl Rogers in which the therapist uses techniques such as active listening within a genuine, accepting, empathetic environment, to facilitate client’s growth Therapist listens, without judging or interpreting, and refrains from directing the client toward certain insights = nondirective therapy Rogers encouraged: genuineness, acceptance, and empathy Active listening- Rogers- echoing, restating, and seeking clarification of what the person expresses (verbally or nonverbally) and acknowledging the expressed feelings Three hints to listen more actively: (1) Paraphrase (2) Invite Clarification (3) Reflect feelings Behavior Therapies Doubt the healing power of self-awareness; assume problem behaviors are the problems Behavior Therapy- applies learning principles to eliminate a troubling behavior View maladaptive symptoms as learned behaviors that can be replaced with constructive behaviors Classical Conditioning Techniques Counter conditioning- pairs the trigger stimulus with a new response that is incompatible with fear Includes exposure therapies and aversive conditioning Exposure Therapies Exposure therapies- behavioral techniques, such as systematic desensitization, that treat anxieties by exposing people (in imagination or actuality) to the things they have feared Systematic desensitization- widely used- a type of counter conditioning that associates a pleasant relaxed state with gradually increasing anxiety triggering stimuli. Commonly used to treat phobias using progressive relaxation the therapist trains you to relax one muscle group after another, until achieve a drowsy state of complete relaxation and comfort therapist asks you to imagine a mildly anxiety arousing situation virtual reality exposure therapy- an anxiety treatment that progressively exposes people to stimulations of their greatest fears, such as airplane flying, spiders, or public speaking Aversive Conditioning aversive conditioning - the goal is substituting negative (aversive) response for a positive response to a harmful stimulus ( such as alcohol). The reverse of systematic desensitization- it seeks an aversion to something the client should avoid Aversive conditioning may work in the short run; in the long run not so much Problem is that cognitions influences conditioning Operant Conditioning Behavior modification- to reinforce desired behaviors and to withhold reinforcement of undesired behaviors or to punish them. Rewards used to modify behavior vary In situational settings, therapists may create a token economy- an operant conditioning procedure in which people earn a token of some sort for exhibiting s desired behavior and can later exchange the tokens for various privileges or treats. Critics of behavior modification express two concerns One: that as for the practical side, these behaviors may disappear when the tokens are discontinued Second: on the ethical side it is not right to control other people’s behavior Cognitive Therapies Cognitive therapists- assume that our thinking colors our feelings that between the event and our responses lies in the mind; cognitive therapy teaches people new, more adaptive ways of thinking and acting If people are miserable they can be helped to change their minds Cognitive Therapy for Depression Aaron Beck- analyzed dreams of people with depression and found recurring negative themes of loss, rejection, and abandonment he sought to reverse clients’ catastrophizing beliefs about themselves, their situations, and their futures often depressed people don’t exhibit the self serving bias and attribute their failures to themselves and attribute their successes to external circumstances. Stress inculcation training- teaching people to restructure their thinking in stressful situations Cognitive behavior therapy- aims to alter the way people act (behavior therapy) and to alter the way they think (cognitive therapy) Make people aware of their irrational negative thinking, to replace it with new ways of thinking and to practice more positive approach in everyday settings Group and Family Therapies Group therapy does not involve the same degree of therapist involvement with each client but it save time and money and is as effective as individual therapy The social context allows people both to discover that other have problems similar to their own and to receive feedback as they try out new ways of behaving Family therapy- treats a family as a system; views an individual’s unwanted behaviors as influenced by or directed at other family members; attempts to guide family members toward positive relationships and improved communication Family therapists work with family groups to heal relationships and to mobilize family resources; aim is to help family members discover the role they play within their family’s social system A wide range of people participate ion self help and support groups On line support groups The grandparent of support groups = Alcohol Anonymous(AA)- has its famous 12 step strategy The more AA meetings patients attend, the greater their alcohol abstinence Evaluating Psychotherapies Before the 1950s the primary mental health providers were psychiatrists Much therapy is done through community mental health programs, which provide outpatient therapy, crisis phone lines, and halfway houses for those making the transition from hospitalization to independent living Is Psychotherapy Effective? Clients’ Perceptions If client’s testimonials were the only measuring stick- could strongly affirm the effectiveness of psychotherapy But there are several reasons as to way client testimonials do not persuade psychotherapy’s skeptics (1) People often enter therapy in crisis (2) Clients may need to believe the therapy was worth the effort- self-justification (3) Clients generally speak kindly of their therapists Testimonials can be misleading- we are prone to selective and biased recall and to making judgments that confirm our beliefs But recall psychology’s most powerful tool for sorting reality from wishful thinking: the control group Clinicians’ Perceptions problem is that clients justify entering psychotherapy by emphasizing their unhappiness, justify leaving therapy by emphasizing their well-being, and stay in touch only if satisfied Because people enter therapy when they are unhappy and leave when they ar less unhappy most therapists testify to therapy’s success- regardless of the treatment Outcome Research Psychologists have turned to controlled research studies The transformation happened when skeptical physicians began to realize that many patients got better on their own, that most fashionable treatments were doing no good, and that sorting fact from superstition required following illness closely—with or without a particular treatment Hans Eysenck- summarize studies showing that 2/3 of those suffering non-psychotic disorders improve markedly after undergoing psychotherapy He also said that with or without psychotherapy roughly 2/3 improve noticeably Randomized Clinical Trials- randomly assign people on a waiting list to therapy or to no therapy; afterward researchers evaluate everyone using tests and the reports of friends and family or of psychologists who don’t know whether therapy was given Metal-analysis- a procedure for statistically combining the conclusions of many different research studies Newer research summaries confirm that psychotherapy works Verdict: those not undergoing therapy often improve, but those undergoing therapy are more likely to improve Psychotherapy is also cost-effective when compared with the greater costs of medical care for psychologically related complaints Annual cost for substance abuse and psychological disorders – a lot Psychotherapy on average is somewhat effective--- this refers to no one therapy in particular Thinking Critically About: “Regressing” from unusual to usual Clients’ and therapists perceptions of therapy’s effectiveness are vulnerable to inflation from two things: (1) placebo effect- power to believe a treatment (2) regression toward the mean- the tendency of unusual events (or emotions) to “regress” (return) toward the average state; extraordinary happenings tend to be followed by ordinary ones We sometimes attribute what may be a normal regression to something we have done Therapy-efficacy research: discerning whether troubled people’s improvement following a particular therapy exceeds what we could expect from the placebo and regression effects, as shown in control groups not receiving the treatment The Relative Effectiveness of Different Therapies There are some elements of effective therapy such as empathy Lists of empirically supported therapies such as: - cognitive therapy, interpersonal therapy, and behavior therapy for depression - cognitive therapy, exposure therapy, and stress inoculation training for anxiety - cognitive behavior therapy fro bulimia - behavior modification for bed wetting new studies confirm cognitive therapy’s effectiveness in coping with depression and reducing suicide risk therapy is most effective when the problem is clear cut Those who suffer less focused problems such as depression and anxiety usually benefit in the short term but often relapse later The more specific the problem the greater the hope Debates over the extent to which clinical practice should be based on scientific evidence or intuitive responses Evaluating Alternative Therapies alternative therapies have no evidence because their proponents and devotees feel no need for controlled research for them personal experience is evidence Eye Movement Desensitization and Reprocessing (EMDR) Francine Shapiro – eye movement desensitization and reprocessing (EDMR)-observed that anxious thoughts vanished as her eyes spontaneously darted about The treatment need take no more than three 90 minute sessions EMDR therapists are applying the technique to other anxiety disorders, such as panic disorder Thousands adore this therapy but thousands more don’t believe in it Skeptics suspect that what is therapeutic is the combination of exposure therapy – repeatedly relieving traumatic memories in a safe and reassuring context Light Exposure Therapy Seasonal affective disorder- aka SAD- for some people especially women and those living far from the equator , the wintertime blahs constitute a form of depression Clinical experience indicated that light exposure could also relieve symptoms associated with wintertime depression Commonalities among Psychotherapies Good therapists have differing perspectives but share a lot in common with other therapists Jerome frank, Marvin Goldfried, Hans Strupp, and Bruce Wampold studied the common ingredients of various therapies and suggest they all offer at least three benefits: hope fro demoralized people, a new perspective on oneself and the world; and an empathetic, trusting, caring relationship Healers- special people to whom others disclose their suffering Hope for Demoralized People People who seek therapy typically feel anxious, depressed, devoid of self esteem, and incapable of turning things around Expectation: with the commitment for the therapy seeker, things can and will get better This belief can act like a placebo and promotes improved morale, new feelings of self-efficiency, and diminished symptoms Improvement is greater for placebo treated people than for untreated people A New Perspective Therapy can offer new experiences and plausible explanations of symptoms and an alternative way of looking at oneself or responding to the world Armed with an new perspective people may approach life with a new attitude An Empathetic, trusting, Caring Relationship All therapist are not all equally effective Effective therapists are empathetic people who seek to understand another’s experience; communicate their care and concern to the client; earn the client’s trust and respect through respectful listening, reassurance, and advice Therapeutic alliance- the emotional bond between therapists and client and is a key aspect of effective therapy Paraprofessionals- other briefly trained people; in some studies they were as effective as trained therapists part of what all therapies offer is hope, a fresh way of looking at life, and an empathetic, caring relationship Culture and Values in Psychotherapy On certain matters of moral and cultural diversity, therapists may differ form one another and from their clients Albert Ellis and Allen Bergin disagree more radically than most therapists on what values are the healthiest They agree on: that psychotherapists’ personal beliefs and values influence their practice; also agree that therapists should divulge their values more openly Value differences also can become significant when a therapist from one culture meets a client from another Difference help explain the reluctance of some minority populations to use mental health services The Biomedical Therapies Physically changing the brain’s functioning by altering its chemistry with drugs, overloading its circuits with electroconvulsive shock, using magnetic impulses to stimulate or dampen its activity, or altering its circuits through psychosurgery Drug Therapies Psychopharmacology- the study of drug effects on mind and behavior Discoveries have revolutionized the treatment of people with sever disorders Almost any therapy treatment including drug therapy is greeted with enthusiasm Enthusiasm diminishes when researchers subtract the rates of (1) normal recovery among untreated people and (2) recovery due to placebo affect, which arises from the positive expectations of patients and mental health workers alike Use double blind technique to measure effectiveness of drugs Antipsychotic Drugs Antipsychotic drugs –calm psychotic patients and dampen responses to irrelevant stimuli Patients exhibiting negative symptoms often don’t respond well to these drugs Clozapine- a drug that enables “awakenings” in people like that and it sometimes helps those who have positive symptoms but have not responded to other drugs Must have regular blood tests when taking this Molecules of antipsychotic drugs are similar enough to molecules of the NT dopamine to occupy its receptor sites and block its activity Proves that an overactive dopamine system contributes to schizophrenia First generation dopamine blocking drugs can produce sluggishness, tremors, and twitches Long term use can produce tardive dyskinesia- a neurotoxic effect involving involuntary movements of facial muscles, tongue and limbs New generation antipsychotic drugs have fewer side effects but they appear hardly more effective and seem to increase the risk of obesity and diabetes One person’s effective dose may be another’s overdose or under dose Antianxiety Drugs Antianxiety agents- depress central nervous system activity; used in combo with psychological therapy it can help a person learn to cope with frightening situations and fear triggering stimuli Criticism of behavior therapies: that they reduce symptoms without resolving underlying problems; this also goes for antianxiety agents May be used as an ongoing treatment though However can cause psychological and physiological dependence Antidepressants Antidepressants- can lift people up from a state of depression; works by increasing the availability of norepinephrine or serotonin, neurotransmitters that elevate arousal and mood and appear scarce during depression Fluoxetine aka Prozac- partially blocks the reabsorption and removal of serotonin from synapses This is called a selective-serotonin-reuptake-inhibitor (SSRIs) Other dual action antidepressants work by blocking the reabsorption/ breakdown of norepinephrine and serotonin Have more potential side effects Full psychological effect of antidepressants takes four weeks One possible reason fro the delay: increased serotonin promotes neurogenisis- the birth of new brain cells, perhaps revering stress induced loss of neurons Antidepressants = not only way to get a lift Can be happier with aerobic exercise, cognitive therapy, and u can use both antidepressants with cognitive therapy Regression to normal is called spontaneous recovery Placebos that mimic the side effects of antidepressants are nearly as effective as the drugs themselves The suicide concern resurface in the earl 21st century with studies indicating that children and adults are at a temporary heightened risk of suicide just after beginning drug treatment Recent studies however show that the long term increase in antidepressant use correlates with a decline in the adolescent suicide rate Mood Stabilizing Medications The simple slat Lithium can be an effective mood stabilizer for those suffering the manic depressive swings of bipolar disorder John Cade discovered this – he thought lithium had calmed excitable guinea pigs when it actually made them sick Realized on patients that they were getting better and that with continued use emotional high and lows typically stabilize We don’t fully understand why lithium works Brain Stimulation Electroconvulsive Therapy Electroconvulsive Therapy (ECT)- a biological therapy for severely depressed patients in which a brief electric current is sent through the brain of an anesthetized patient Usually limit ECT to treatment of severe depression Don’t really know how it works Maybe the shock induced seizures cause the brain to react by calming neural centers where the over activity produces depression ECT reduces suicidal thoughts and is credited with saving many from suicide ECT- treated patients are vulnerable to relapse Alternatives to ECT Some patients with chronic depression have found relief through a chest implant that intermittently stimulates the vagus nerve, which sends signals to the brain’ mood- related limbic system Depressed moods seem to improve when repeated pulses surge through a magnetic coil held close to a person’s skull- magnetic energy only penetrates to the brain’s surface This procedure is called repetitive transcranial magnetic stimulation (rTMS)- and is performed on wide awake patients from 20-30 minutes four 2- 4 weeks Produces no seizures, no memory loss, or other side effects Psychosurgery Psychosurgery- surgery that removes or destroys brain tissue; the most drastic and least used biomedical intervention for changing behavior Lobotomy- Egas Moniz- best known psychosurgical operation; found that cutting the nerves connecting the frontal lobes with the emotion controlling centers of the inner brain calmed uncontrollably emotional and violent patients It usually produced a permanently lethargic, immature, impulsive personality Procedure like these are irreversible so doctors go to them only as a last resort Preventing Psychological Disorders We could interpret many psycho. Disorders as understandable responses to a disturbing and stressful society Preventive mental health is upstream work: it seeks to prevent psycho. Casualties by identifying and alleviating the conditions that cause them George Albee believes there is abundant evidence that poverty, meaningless work, constant criticism, unemployment, racism, and sexism undermine people’s sense of competence, personal control, and self esteem. He says we care too much about preventing psycho. Casualties should therefore support programs that alleviate poverty, discrimination, and other demoralizing situations Biological events: stress affects body chemistry and health and chemical imbalances can produce disorders like depression and schizophrenia