Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
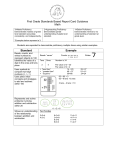
200- 2 TENS Intake TENS UNIT INTAKE FORM Date written order was received. ___________________________ Do not deliver prior to receiving written order. Patient’s diagnosis __________________________ Not covered if ordered for: 1. Headache 2. Abdominal pain 3. Pelvic (hip) pain What type of tens unit? 2 Lead 4. TMJ 4 Lead If 4 leads are ordered: Why 2 are leads insufficient to meet the patient’s needs. REASON: _______________________________________ We must obtain written reason from physician or qualified professional. Is the tens unit being ordered for post operative pain? Yes No If yes: Date of surgery: ______________________ Medical necessity for post-op pain is limited to 30 days from surgery date. --OR- Does patient have chronic, intractable pain? Yes No If yes: How long has patient had pain? ___________________ Pain must be present for at least 3 months to qualify. Is there documentation of other types of medications and/or therapies that have been tried and failed? Yes No--If No patient will not qualify. Trial/ rental will be covered for at least 30 days not to exceed 2 months. Electrodes are not paid separately during the rental period. Purchase can be authorized after the trial period (31st or 61st day). Rev 7/2005