Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
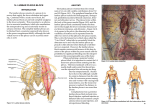
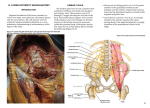
Anterior approaches of the Lumbar Plexus Matthias Desmet az|groeninge Anatomy of the Lumbar plexus Lumbar plexus (L1-L4): Ilio-hypogastric n. Ilio-inguinal n. Genitofemoral n. Femoral n. Lateral femoral cutaneous n. Obturator n. Innervation of the hip? Anterior Posterior Femoral N. Sciatic N. Lateral-Anterior Superior Superior Gluteal N. Obturator N. Lateral Medial N. to Quadratus Femoris Inferior Birnbaum et al. Surg Rad Anat 1997 Aiming at the lumbar plexus… Posterior approaches: • • • • L4 approach by Capdevilla L4-L5 approach by Winnie L4-L5 approach by Chayen L3 approach by Parkinson • Shamrock approach by Sauter • USG approach by Karmaker Awad et al. RAPM 2005 Sauter et al. EJA 2015 Karmaker et al. RAPM 2015 Posterior Approaches of the Lumbar Plexus. • Landmark based or Ultrasound Guided • Technically challenging • Major Adverse Effects: • • • • • Epidural spread: 1-16% Spinal Injection Intravascular Injection Infection Hematoma incl. subcapsular renal hematoma Awad et al. RAPM 2005 Sauter et al. EJA 2015 Karmaker et al. RAPM 2015 Anterior approach of the lumbar plexus Winnie et al Anesth Analg 1973 CONCLUSION: No involvement of the proximal and posterior portions of the obturator nerve was observed, nor was there any cephalad spread that could have resulted in a lumbar plexus blockade. Marhofer P et al. Anesth Analg 2000 The fascia iliaca compartment block 1989 Dalens et al. Anesth Analg 1989 Despite considerable cephalad spread, there was no extension of injectate into the tissue plane reaching the ON in any patient. Adductor strength of the femur at the hip was normal (5/5) in all patients. Thus, none of the 10 patients manifested objective evidence for ON block. Swenson et al. J Clin Anesth 2015 Hip Fractures? Clinical utility of FICB? • Reduction in pain scores at rest and on mobilisation • Reduction in analgesic consumption • Decreased incidence of postoperative complications All studies reported reductions in pain intensity with femoral nerve blocks. All but one study reported decreased rescue analgesia requirements. Two studies found a decreased risk of adverse events such as respiratory and cardiac complications. Riddell et al. CJEM 2016 Newman et al. Anesthesia 2013 Longitudinal supra-inguinal FICB? • Cadaver study. • MRI Study in volunteers. • Clinical trial assessing the clinical utility. Cadaver study: Step up technique with different volumes of dye. 20-30 mL: inconsistent spread of dye, no involvement of ON. 40-50 mL: consistent spread of dye, involvement of ON. Vermeylen et al. unpublished data Cryogenic preservation technique: Spread posterior of psoas muscle. MRI study on volunteers • 10 volunteers. • Bilateral FICB: classical versus longitudinal supra-inguinal approach. • MR imaging to assess spread of 40ml LA. • Data analysis ongoing Vermeylen K, Desmet M et al. Unpublished data Transverse FICB Longitudinal suprainguinal FICB Longitudinal suprainguinal FICB Transverse FICB L4 Transverse FICB Longitudinal suprainguinal FICB • Randomized controlled, double blinded trial. • 88 patients, for anterior approach THA under GA. • Longitudinal Supra-Inguinal Fascia Compartment Block vs Control Results: Morphine consumption. 45% morphine reduction at 48 hours Results: Pain scores Results: Sensory and Motor Evaluation Results: Safety? Total Ropivacaine Levels <4.3mg/L Free Ropivacaine Levels <0.56mg/L Conclusions: • Longitudinal supra-inguinal FICB is a promising approach of the LP. • Easy to perform with a high succes rate. • Safe in terms of LA toxicity. • More research needed. A Big Thank You!!!