Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
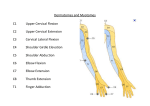
Examination of the Shoulder The preliminaries: Introduce yourself to patient, ask for permission to examine. Ensure adequate exposure but consider patient modesty also. Ensure good lighting, and good positioning of bed. In supraspinatus impingement or tear, passive range is greater than active range as active range is limited by pain and/or weakness; limitation is usually only in one movement e.g. abduction. In frozen shoulder, passive and active range of movements are equally restricted, and usually in more than one type of movement. LOOK 1. General appearance and vitals – any pallor, what is the BP, and HR. 2. Scars over shoulder, in axilla 3. Swelling - Bump(s) over sternoclavicular joint, clavicle, acromioclavicular joint - Effusion points in the axilla – remember to look 4. Sinuses 5. NOTE: for assessment of range of abduction and flexion, it is important to fix the scapula and note the glenohumeral joint movement; increased scapulothoracic movement may compensate for decreased mobility at the glenohumeral joint. a. Deformity – asymmetry between two shoulders - Foreshortening of the shoulder joint indicates previous clavicular fracture, acromioclavicular joint problem Abduction (raise both arms to meet above the head) – also assess “painful arc” of 60 to 120 degrees for supraspinatus impingement. b. Adduction (cross-shoulder – get patient to touch other shoulder with hand, observe how far the hand can reach). 6. Discolouration – redness, bruising, etc c. Flexion and extension. 7. Muscle wasting – squaring of the shoulder (deltoids); hollowing of supra- or infraspinous fossa d. Internal rotation (place hands behind back and see how which level the patient’s extended thumb can reach e.g. inferior angle of scapula – T7). 1. Warmth e. 2. Tenderness - Start from SC joint, go along clavicle to AC joint, then ballot AC joint - Follow back to spine of scapula, and palpate in supraspinous and infraspinous fossae for tenderness - Locate coracoid process anteriorly, palpate that (short head of biceps, coracobrachialis) - Head of humerus - Greater tuberosity (particularly supraspinatus insertion) - Bicipital groove – tendon of long head of biceps External rotation (with elbows tucked close to sides and flexed 90 degrees, rotate outwards). FEEL MOVE 1. Range of movements: - Get patient to do actively; if there is any restriction of a particular movement, proceed to assess passive range – this assesses if the decrease in range is due to pain, joint stiffness or muscle weakness. 2. Power of rotator cuff muscles: - Abduction (supraspinatus): Keep the shoulder in 30 degrees flexion so that the humerus is in line with the scapula (isolates supraspinatus?) and then place the shoulder in 30 degree abduction with the elbow flexed completely. Examiner presses down on patient’s elbow while patient resists. - Flexion and extension. - Internal rotation (subscapularis) – Gerber’s lift-off test: get patient to place hands behind back, then examiner presses the hand against the patient’s back while patient attempts to lift his hand off. If patient is unable to place hands behind back due to restricted ROM, perform the belly press test, where patient presses palms against his or her abdomen and examiner attempts to pull the hand off the abdomen. - External rotation (infraspinatus and teres minor). SPECIAL TESTS Supraspinatus impingment tests: 1. Painful arc (between 60 to 120 degrees of passive abduction classically, as greater tuberosity hits acromion and the supraspinatus is caught in between). 2. Jobe’s test (or beer can test) – with the arm abducted 90 degrees and in neutral rotation, internally rotate the arm, like inverting a beer can held in the hand. 3. Hawkin’s test – with the arm flexed 90 degrees and elbow flexed 90 degrees, internally rotate the arm. Supraspinatus tear: - Abduction paradox and Drop-off sign – patient is unable to initiate abduction of the shoulder, but when arm is passively abducted to more than 90 degrees, he or she is able to maintain abduction by deltoid action. When the arm is passively adducted to less than 90 degrees of abduction and the examiner lets go of the arm, the arm will fall to the patient’s side as he is unable to maintain the abduction. Biceps tendinitis (tendon of long head of biceps) 1. Speed’s test – with elbow fully extended and forearm supinated, the patient flexes his shoulder against resistance on the arm; test is positive when there is pain localised to the bicipital groove. 2. Yegarson’s test – with elbow flexed to 90 degrees and forearm pronated, patient attempts to supinate forearm against resistance; test is positive when there is pain localised to the bicipital groove. FINISH with assessment of neurovascular status of the upper limb, and examine the cervical spine. Examination of the Hand The preliminaries: Introduce yourself to patient, ask for permission to examine. Ensure adequate exposure, remove all accessories. Ensure good lighting, and good positioning by placing patient’s hands on a pillow. The focus of hand examination is the 5 different tissues in the hand – (1) Skin and subcutaneous tissue; (2) Muscle and tendon; (3) Blood vessels; (4) Nerves; and (5) Bones and joints. Note which tissue(s) the pathology lies in. RADIAL NERVE 2. MOVEMENTS 1. LOOK Observe hands in supinated and pronated positions (palmar and dorsal surfaces) 1. Scars 2. Swellings - Lumps and bumps on the hand – describe site, size, shape, borders, surface, consistency, fluctuance if any, transilluminability, mobility (along tendon course or perpendicular to the course), increase or decrease in size with flexion - Common DDx of any lump: ganglion, PVNS, implantation dermoid, pyogenic granuloma 3. Sinuses 4. Deformity Loss of hand cascade (little finger is most flexed, index finger least flexed, in resting position of hand) - Joint contractures if any - Rheumatoid features 5. Discolouration 6. Muscle wasting Thenar eminence, hypothenar eminence Wasting of the interossei guttering Feel joints of hands for: Tenderness Nodules Joint line irregularity Subluxation Quick screening tests - With forearm supinated (palms face-up), get patient to fully flex fingers – tests patency of flexor tendons and nerves. - - 2. With forearm pronated (dorsum face-up), observe for any wrist and/or finger drop, then get patient to extend wrist and fingers fully – tests patency of ECRB, ECRL and ECU for wrist, EDC for the MCP joints, intrinsics for the PIP and DIP joints. With elbows tucked in close to patient’s sides, get patient to pronate and supinate forearm to check range of movement – assesses proximal and distal radioulnar joint, and biceps action. Assessment of active and passive range of movements - If active range of movements < passive range of movements, there is muscle weakness (nerve palsy), tendon rupture, or tendon adhesion to surrounding tissue. - If passive range of movement is restricted, there is joint contracture. - Symmetry of movements is a useful guide to whether there is abnormality. NERVE TESTING 3 impt functions: SENSORY, MOTOR, and AUTONOMIC FEEL 1. Tenderness over: - Anatomical snuffbox – base (scaphoid); borders (EPL, APL, EPB) - Distal radio-ulnar joint – check for subluxation (piano-key sign) - Lister’s tubercle on dorsum of distal radius scapholunate junction is just distal to this landmark - Radial and ulnar styloids - Sensory: pinprick sensation over area supplied by nerve; most sensitive testing is using 2 point discrimination. - Motor: Power of muscle(s) supplied by nerve. - Autonomic: Skin warmth, dryness. Use a plastic pen and rub over finger supplied by that nerve; normally there should be feeling of friction, but if autonomic supply is lost the pen will slide smoothly over the skin. I. Sensory supply: - Dorsal surface of radial 3½ digits and corresponding area of dorsum of hand. - Test the dorsal aspect of the first web space. II. Motor supply: - The most distal extensor muscle supplied by the posterior interosseous nerve is the extensor indicis propius (EIP) but this cannot be tested accurately due to the tendon slip from EDC to the index finger. - Instead, the next most distal muscle, the EPL, is tested instead – place the hand flat on a table and get the patient to lift his thumb off the table (retropulsion). If EPL function is intact all other muscles supplied by radial nerve should be intact. - EDC testing – get patient to extend MCP joints and flex the PIP and DIP joints (like making a claw) to isolate action of the EDC. - Higher lesions e.g. shaft of humerus fracture result in paralysis of the wrist extensors (ECRL, ECRB, ECU) and wrist-drop results i.e. low lesions of radial nerve do not result in wrist-drop, so be careful. - Triceps function is usually preserved unless lesion is very high up; shaft of humerus # usually does not result in triceps paralysis. MEDIAN NERVE I. Sensory supply: - Palmar surface of radial 3½ digits and corresponding area of palm, over thenar eminence - Cutaneous branch to thenar eminence is given off before carpal tunnel, thus there is no loss of sensation over the thenar eminence in CTS - Test tip of index and middle fingers and thumb, and thenar eminence II. Motor supply: - Intrinsics – test the abductor pollicis brevis (APB) by getting patient to abduct thumb (in a plane perpendicular to the plane of the palm) against resistance. The APB is the thenar muscle that is solely supplied by the median n. 99% of the time; the other two muscles may receive cross-supply from the ulnar n. - - Anterior interosseous nerve supplies FPL, pronator quadratus and radial half of FDP Testing FDP: Fix middle phalanx of index finger and get patient to flex the DIPJ Testing FPL: Flexion of the IP joint of the thumb while fixing the proximal phalanx OK sign: Ask patient to make an “OK” sign by forming a circle with the thumb and index finger; this action involves flexion of DIPJ of index finger and IPJ of thumb, so if there is anterior interosseous nerve palsy these two joints are extended (like holding a needle) and the OK sign cannot be made properly. The FDS is still intact, however, since the patient is able to flex his PIPJ of the index finger. Testing the FDS and its tendons (supplied by median nerve proper): Fix the distal phalanges of the fingers adjacent to the finger being tested, and get patient to flex the PIP joint of the finger being tested. of the hand. This tests action of adductor pollicis, and if there is paralysis of this muscle the patient will attempt to compensate by flexing the thumb to hold the paper in place. Compare to normal side. Wartenburg sign – ask patient to hold fingers adducted and extended; the little finger will become abducted in paralysis of the intrinsics as the adduction ability of the palmar interossei is lost, and the extension action of the extensor digiti minimi (EDM) pulls the little finger into abduction. - III. Other tests: - Tinel’s sign: tap on the ulnar nerve as it runs behind medial epicondyle; if patient has had operation to anteriorly transpose ulnar nerve, then tap anterior to the medial epicondyle. Positive when there are shooting pains along the course of the ulnar nerve. - III. Others: - Tinel’s sign: tap over proximal edge of the palm, where the carpal tunnel is located. Positive sign is when there is shooting pain and numbness radiating towards the radial 3.5 digits. - Phalen’s test: examiner’s thumb is placed over the carpal tunnel and patient’s wrist is flexed for 30 seconds. Positive when numbness over radial 3.5 digits is reproduced by this test. ULNAR NERVE I. Sensory supply - Dorsal and palmar surfaces of ulnar 1½ fingers and corresponding areas of palm and dorsum of hand - Cutaneous branch to the dorsum of the hand is given off before the wrist, so there is sparing of sensation over that area in an ulnar nerve lesion at the wrist. - Test the little finger, over the hypothenar eminence, and over medial side of the dorsum. II. Motor supply - Intrinsics Test the first dorsal interosseous – abduction of the index finger against resistance Froment’s sign – get patient to hold on to a piece of paper placed between thumb and radial border FDP of the little finger: hold middle phalanx of little finger and get patient to flex the DIP joint of the finger. Ulnar nerve subluxation: place a finger on the ulnar nerve and slowly passively flex patient’s elbow, feeling for anterior subluxation of the ulnar nerve VASCULAR EXAMINATION - Colour of the skin (pink, or dusky, or pale) - Capillary refill (should be <2 seconds) - Temperature - Tissue turgour - Allen’s test is optional: Get patient to clench fist tightly, place fingers of each hand on radial and ulnar arteries respectively, then get patient to open hand and examiner releases one hand, noting the time that is required for the hand to turn pink. Then release the other side to allow hand to reperfuse, and repeat for the other artery. OTHER TESTS Finklestein’s test – for DeQuervain’s tenosynovitis Patient closes fist with thumb tucked under clenched fingers. Holding arm outstretched with forearm in neutral rotation i.e. thumb facing upwards, patient is told to ulnar deviate the wrist. Positive test is when there is pain localised to the radial styloid region. If done properly, the Finklestein’s test is a very sensitive test for DeQuervain’s. FINISH with examination of the cervical spine. APPROACH TO THE HAND EXAMINATION: Start off with a quick screen – expose both hands up to elbow, look at the plantar aspect with hands open, then ask patient to close hand, the look at the dorsal aspect By this time you should have ascertained the problem: 1. A lump 2. Deformity – arthritis 3. Nerve palsy Approach to nerve palsies: 1. Which nerve is involved? 2. What level is the nerve involved? 3. What is the cause? Ulnar nerve Look: Claw hand Wasting of the first dorsal interosseous, guttering Test: Abduction of index finger (first dorsal interosseous) Adduction (cross the first two fingers) FDP of the little finger Froment’s sign Sensation to little finger, hypothenar eminence Site of lesion: FDP and sensation to hypothenar lost in elbow lesion, preserved in lesion at wrist Cause: Carrying angle of elbow Lacerations over medial aspect of elbow Thickened ulnar nerve Ulnar nerve subluxation Median nerve Look: Wasting of thenar eminence Test: FPB (abducting thumb) FDP and FPL (making OK sign) FDS (flexion of PIPJ) Sensation to index finger, thenar eminence Site of lesion: Carpal tunnel spares thenar sensation, FDP, FPL, FDS but affects FPB; AIN lesion hits FDP, FPL; high lesion loses all Cause: Tinel’s and Phalen’s at carpal tunnel Radial nerve Look: Finger drop with or without wrist drop Test: EPL (retropulsion of thumb) Extension of fingers (EDC) Extension of wrist (ECR, ECU) Extension of elbow (triceps brachii) Sensation over first web space Site of lesion: PIN lesion will cause finger drop but not wrist drop and no sensory loss; spiral groove injury will cause wrist drop and sensory loss Cause: Humeral neck fracture most common Examination of the Hip The preliminaries: Introduce yourself to patient, ask for permission to examine. Ensure adequate exposure but consider patient modesty also. Ensure good lighting, and good positioning of bed. With patient lying supine, knees fully extended: 3. Deformity of the hip – fixed adduction or abduction deformities; asymmetry in attitude of the limb 4. Obvious swelling(s) - Hernia can cause hip pain – look for it GAIT AND RELATED TESTS 1. 2. Get patient to walk a distance – notice if there is any obvious antalgic or Trendelenburg gait, of if one of the limbs appear shorter than the other Types of gait: - Antalgic – shorter stance phase on painful side - Trendelenburg – when supporting body weight on abnormal side, hip sags on the opposite side and patient thrusts torso towards affected side - Weak gluteus maximus – patient leans backwards to keep hip in full extension when the weak side is in stance phase - Hand-to-knee – patient places hand on thigh to keep knee extended due to weak quadriceps - High-stepping gait – due to foot drop (common peroneal nerve palsy) Trendelenburg test: - Get patient to stand in front of you and place both hands on top of your own (palms down on your palms up) - Then make patient stand on one foot at a time, lifting the other off the floor - If the side that the patient is supporting his weight on has a pathology, the patient’s hip will sag towards the opposite side and his hand will press harder on that side to lever himself Causes of positive Trendelenburg test: - Fulcrum problems e.g. hip OA, AVN - Lever arm problems e.g. NOF#, coxa vara - Effort problems e.g. weak abductors LOOK With patient standing: 8. Scars 9. Swelling 10. Sinuses – in the gluteal folds, make sure to check 11. Discolouration – redness, bruising, etc 12. Muscle wasting – gluteal muscles FEEL o Feel for temperature – any increased warmth o Palpate for tenderness – locate hip joint 2cm below and lateral to midpoint of inguinal ligament; greater trochanter MOVE 3. Thomas’ Test for fixed flexion deformity of the hip - Place patient’s legs at 90 degree knee flexion - Then place your hand under patient’s lumbar region - Get patient to flex one leg at the hip until the lumbar lordosis is obliterated (back pressing your hand to the bed) and then ask patient to hold on to the flexed leg at the knee - Ask patient to fully extend the other leg to see if there is any fixed flexion of the hip - Repeat with the other side - Be consistent in performing the test – amount of pressure of lumbar region on the hand should be equal when testing either side NOTE: if patient has a knee contracture, shift him such that his knee joint lies over the edge of the bed, to accurately assess for FFD of the hip 4. Range of movements: - Hip movements are mostly assessed passively - While during Thomas’ test, also assess degree of full hip flexion on either side (normal is 140 degrees flexion) - Abduction and adduction – place hand on the ASIS to assess movement of the hip joint when the pelvis is not moving (normal range is 45 degrees abduction and 30 degrees adduction) - External and internal rotation – flex hip and knee to 90 degrees each, place left hand on knee pressing downwards to fix pelvis (normal is 50 degrees external rotation, 40 degrees internal rotation) NOTE: If patient cannot flex hip due to pain, internal and external rotation of the hip can be assess with patient in prone position and the knee flexed - Turn patient to the prone position to assess extension of the hip LIMB LENGTH MEASUREMENT Square the pelvis for true length measurement; ensure axes of both lower limbs are at right angles to the line joining the two ASIS. If not possible to square pelvis due to contracture on one side then arrange the other limb in the same position when measuring true length for that limb. True length: - Locate ASIS by feeling laterally from the pubic tubercle; the ASIS is the first bony prominence that the hand feels - Measure from ASIS to medial malleolus (use the same relative point on the malleolus on either side e.g. superior border, midpoint, etc) - If one side has an abduction contracture, then place the other leg in the same relative position when measuring true length; same for other deformities Relative length - For measurement of relative limb length just ask patient to adopt the most comfortable position: “shoulders above hip above feet” - Locate xiphoid process and then measure from that point to the medial malleolus on either side Contractures and apparent length discrepancy - Adduction deformity results in shortening of the abnormal side - Abduction deformity results in lengthening of the abnormal side Galeazzi’s test Place the lower limbs side by side with knees flexed 90 degrees, with the heels in line This screening test helps to assess if the shortening is due to femur or tibia or both Bryant’s triangle If shortening is in the femur, it is important to assess if the shortening is above or below the greater trochanter Bryant’s triangle is formed by a line joining the ASIS and the greater trochanter, a line dropped vertically from the ASIS, and a line running horizontally across from the greater trochanter Shortening of the horizontal line on one side as compared to the other indicates shortening above the greater trochanter FINISH with examination of the neurovascular status of the lower limb, and examination of the spine and knee joints Examination of the Knee The preliminaries: Introduce yourself to patient, ask for permission to examine. Ensure adequate exposure but consider patient modesty also. Ensure good lighting, and good positioning of bed. 8. Feel for temperature gradient over the knee joint, and any difference in temperature compared to the other knee 9. Feel the articular surface of the patella for tenderness, osteophytes. LOOK With patient standing: 10. Other swellings e.g. cysts around the knee, osteophytes in OA knee 13. General appearance and vitals – any pallor, what is the BP, and HR. 14. Deformity – varus or valgus - measure intercondylar distance (normal <5cm) and intermalleolar distance (normal < 2cm) 1. 16. Swelling - effusion w/ obliteratn of medial parapatellar fossa - cyst e.g. Baker’s cyst over popliteal fossa 18. Discolouration – redness, bruising, etc 5. 6. Fixed flexion deformity of the knee - Ask patient to push down on examiner’s hand placed in the popliteal fossa to see if patient is able to press hand against bed 5. - 7. Fluid shift (sensitive for small amounts of fluid) – stroke medial parapatellar fossa to empty it of fluid, then press on lateral side to see if medial fossa fills again Patellar ballottement/tap – with left hand pressing on suprapatellar pouch, use thumb and index finger of right hand to press down on patellar; test is positive when patellar hits femur with a tap Muscle wasting over quadriceps (vastus medialis is most prominent) - Measure girth of quadriceps 10cm (or 4 fingerbreadths) about the superior border of the patella – “objective assessment of wasting”; significant if difference is greater than 2 cm. Palpate for tenderness with one thumb: - Tibial tuberosity - Patellar tendon - Around either side of the patella - Quadriceps tendon around the superior border of the patella - Medial and lateral joint lines, one at a time - Femoral condyles Active range of movements: - Get patient to flex knee all the way and then extend, looking for any restriction of full flexion or extension 6. Passive range of movements: - If patient has restricted range of movements, assess if there is a joint contracture or muscle weakness 7. Crepitus - Feel with hand over patella during passive movement Effusion – obliteration of medial parapatellar fossa - 4. Collateral ligaments test in full extension (where capsular elements and other ligaments are also taut and restrict displacement) and in 30 degrees flexion (where only the MCL and LCL are responsible for preventing displacement 5. McMurray’s test - Start with knee in full flexion - To test medial meniscus, externally rotate tibia with your right hand at the ankle, and apply valgus force at the knee with your left hand, then extend the knee - To test lateral meniscus, internally rotate tibia and apply varus force at the knee, then extend - Repeat the test, looking out for palpable or audible click in the knee during extension 6. Other special tests that can be done: - Quadriceps active test for PCL – with patient’s knee joint in 90 degree flexion and examiner sitting on patient’s foot, get patient to contract quadriceps muscle; positive when tibia shifts forward eliminating the posterior sag appearance MOVE 19. Muscle wasting – quadriceps LOOK AND FEEL With patient lying supine, knees fully extended: Lachman’s test With knee in 20-30 degrees flexion, place left hand on thigh pressing downwards, and right hand under the proximal calf with thumb over the joint line pulling the tibia towards you Also testing for ACL, but more sensitive test With knee flexed to 90 degrees: 15. Scars over anterior and posterior aspect of knee 17. Sinuses 3. SPECIAL TESTS With legs placed in 90 degrees flexion and aligned (heels in the same line): 1. Posterior sag sign - look for posterior sag of tibial tuberosity on the femoral condyles posterior cruciate injury 2. Anterior drawer test - Sit on patient’s foot, use both hands to splint the hamstrings, with thumbs on the joint line, and pull towards you - In ACL tear, there will be no end-point on pulling forward - Pivot shift for ACL – with lower limb adducted and knee extended, patient is told to relax and the leg is internally rotated with valgus force applied to the knee, and then flexed; positive when tibia suddenly shifts forward on femur with a click sound (NOTE: test is painful, thus don’t do it during exam) - Patellar apprehension test for recurrent patellar dislocation – push the patella laterally while flexing and extending the knee joint; positive when patient feels like patella is about to dislocate FINISH with assessment of neurovascular status of the lower limb, and examine the hip and ankle joints for any pathology. Examination of the Cervical Spine The preliminaries: Introduce yourself to patient, ask for permission to examine. Ensure adequate exposure but consider patient modesty also. Ensure good lighting, and good positioning of bed. LOOK 20. General appearance and vitals – any pallor, what is the BP, and HR. 21. Deformity – namely tilting of the head (‘wry neck’) - Causes: torticollis (congenital), PID, inflamed neck glands, cerebellar dysfunction, ophthalmologic disorders, congenital scoliosis, atlanto-axial rotatory dislocation, etc. SPECIAL TESTS o For cervical spondylosis: 1. Spurling’s and Davidson’s tests - Spurling’s: Active extension, lateral flexion and rotation of patient’s neck towards the affected side with axial pressure results in reproduction of radicular symptoms e.g. shooting pains down the arm, numbness and weakness. - Davidson’s: Subsequent abduction of the arm on the affected side (with neck still extended, laterally flexed and rotated) results in relief of the radicular symptoms. 2. 22. (Scars, sinuses, swellings) - E.g. cervical lymph nodes FEEL 11. Palpate for tenderness along spinous processes and interspinous ligaments - At the same time palpate for any step deformity (high-grade listhesis), and ligamentous gap (more applicable for trauma). 12. ‘Trigger points’ - Points along the neck musculature that are extremely tender with radiation; reproduces patient’s usual pain symptoms (myofascial pain syndrome?). o o 13. Palpate paravertebral muscles for spasm MOVE 8. 9. Flexion-extension: - 50% of this movement occurs at the atlanto-occipital junction. - In flexion, the patient’s chin should touch the chest. - In extension, the line joining the patient’s chin to the posterior occipital protuberance (occipitomental line) should form an angle of at least 45 degrees to the horizontal (usually more than 60 in young patients) Lateral flexion: - Check symmetry of movements 10. Rotation - 50% of this movement occurs at the atlanto-axial joint - As with lateral flexion, check for symmetry of movements on both sides Motor function 4. Sensory function – Important to compare with chin and not chest since pathology is in the cervical region and the chest belongs to thoracic dermatomes. 5. Proprioception – big thumb 6. Cerebellar function – dysmetria, dysdiadochokinesia 7. Myelopathic hand: (i) Thenar atrophy (ii) Hoffmann’s sign - The examiner holds the patient’s middle finger between thumb and index finger (hold patient’s right hand with examiner’s left hand, index finger of examiner on volar surface of patient’s finger and thumb over dorsal surface) and flicks the patient’s distal phalanx downwards with his thumb. - Positive sign is when there is reflex flexion of the thumb and index finger of the patient. Cervical compression and distraction - Axial loading of the cervical spine results in radicular symptoms, especially while performing the Spurling’s test. - Distraction of the neck (pull the head superiorly) relieves the symptoms. For cervical myelopathy: - Lhermitte’s sign: When patient is asked to actively flex his or her neck, there are electric shock-like sensations that run down the centre of the patient’s back and shoot into the limbs. For thoracic outlet syndrome: - Adson’s manoeuvre: With one hand palpating the patient’s radial pulse, get the patient to extend his neck actively and then rotate it towards the side being tested. Positive result (indicating interscalene compression of the subclavian neurovascular bundle) is when there is diminished pulse, sometimes with distal pain in the affected upper limb. NEUROLOGICAL EXAMINATION (esp. if susp myelopathy) UPPER LIMB: 1. Tone, clonus 2. 3. Reflexes – biceps, triceps, brachioradialis - If the cervical myelopathy occurs at C5 or C6 the ‘inverted supinator reflex’ is present – this is where there is diminished elbow flexion but increased finger flexion on tapping the brachioradialis tendon due to spastic finger flexors; this is associated with hyper-reflexic triceps jerk. - For cervical involvement above C5, elicit Shimizu’s sign (scapulo-humeral reflex) by tapping on spine of scapula or acromion with a tendon hammer; the reflex is hyperactive when the scapula elevates or the humerus becomes abducted. (iii) Grip and release test - Ask patient to quickly flex fingers into a fist and extend, repeatedly, to accomplish 20 cycles in 10 seconds. - In patients with cervical myelopathy the movement is slow, difficult and incomplete. (iv) Finger escape sign - When patient is asked to keep fingers adducted and extended, the ulnar two fingers drift into flexion and abduction within 30 seconds. LOWER LIMB 1. Tone, clonus - Usually there is increased tone in the lower limbs in cervical myelopathy. 2. Reflexes – Knee jerk, ankle jerk, plantar reflexes - Usually hyper-reflexic in cervical myelopathy. 3. Motor - Decreased in cervical myelopathy. 4. Sensation - Decreased in cervical myelopathy. 5. Proprioception and cerebellar function - Gait is usually broad-based and clumsy, check Romberg’s. PR EXAMINATION For saddle anaesthesia, anal wink reflex, anal tone. Examination of the Thoracolumbosacral Spine The preliminaries: Introduce yourself to patient, ask for permission to examine. Ensure adequate exposure but consider patient modesty also. Ensure good lighting, and good positioning of bed. LOOK With patient standing: 23. General appearance and vitals – any pallor, what is the BP, and HR. 24. Scars over back 25. Swelling - E.g. meningocoele, visible spasm of paravertebral muscles, lumps and bumps 26. Sinuses - Over lumbar triangle of Petit (bordered by latissiumus dorsi, iliac crest, and external oblique), or groin region for pus tracking along psoas 27. Deformity - Cervical spine: torticollis, flexion, hyperextension - - Thoracic spine: Kyphosis – angular (gibbus, caused by infection like TB), or smooth (caused by Scheuermann’s disease in adolescents, or multiple osteoporotic compression fractures in old ladies) Scoliosis – with rib hump; note side of curve convexity 15. Percuss for tenderness - Pain on percussion relates to pathology in the antr vert body, may indicate infection or tumour - Do a renal punch to exclude renal pathology 29. Muscle wasting – not much to see actually FEEL 14. Palpate for tenderness along spinous processes - At the same time palpate for any step deformity (high-grade listhesis), and ligamentous gap (more applicable for trauma) 1. MOVE (mostly passive) NOTE: There are no “normal” range of movements in the spine, but assessment of ROM helps establish a baseline range that is useful for future monitoring of disease progress or efficacy of treatment 11. Flexion-extension: - For flexion, do Schoeber’s test for spinal excursion – mark the level of the PSIS and a point 10 cm about it – the increase in distance when bending forwards should be >5cm. 2. Passive dorsiflexion - Following SLR positive, lower the limb a little such that there is no more radicular pain, then passively dorsiflex the patient’s ankle - Is more specific than a simple SLR, because positive SLR can be due to causes other than PID e.g. hamstring tightness 3. Bowstringing test - With hip flexed ~100 degrees, knee flexed 80-90 degrees, locate the biceps femoris tendon on the lateral side of the popliteal fossa - Press on the tendon as a control test – there should not be any pain - Subsequently press medial to the tendon (within the lateral region of the popliteal fossa) where the common peroneal nerve runs - Positive test is not just when there is pain at then point of pressure, but when the pain radiates proximally and/or distally from the point of pressure. - Most useful confirmatory test of nerve rt tension 4. Lasegue test - With knee and hip flexed to 90 degrees each, slowly extend knee and look out for radicular pain - This test is not commonly performed 12. Lateral flexion: - If patient can reach below knees should be normal 13. Rotation - Make patient sit down to fix pelvis, then rotate - Angle between line joining shoulders and line joining ASIS is the extent of rotation NEUROVASCULAR EXAMINATION 7. Reflexes - Knee jerk, ankle jerk, plantar reflex 8. Sensation by dermatome - Anterior thigh for L2 - Anterior aspect of knee for L3 - Medial surface of leg for L4 - Big toe dorsum for L5 - Lateral aspect of heel for S1 - Popliteal fossa for S2 9. Power - Particularly knee extension for L4; ankle and big toe dorsiflexion for L5; ankle and big toe plantarflexion for S1 10. Pulses 11. PR - Saddle anaesthesia (S3, 4, 5) - Inspect anal orifice for tone (“crow’s feet”) - Anal wink reflex – scratch perianal skin and watch for anal wink - Put finger in rectum to assess anal tone Straight leg raising test (SLR) Keeping the knee extended, slowly raise the leg being tested, checking patient’s face to assess pain - Stop when patient complains of pain – positive SLR is when there is pain radiating into the lower limb (radicular pain) - Take note of angle at which radicular pain occurs - Also assess cross-SLR – patient complains of radicular pain in the affected side when the normal lower limb is being raised this indicates a large central PID? And is quite specific for PID? - 16. Palpate paravertebral muscles for spasm Lumbar spine: Transverse lumbar crease and hyperextension – high-grade spondylolisthesis Scoliosis if any 28. Discolouration – bruising, hairy patch over sacrum, café-au-lait spots, neurofibromata NERVE ROOT TENSION SIGNS FABER TEST - for sacroilitis – in young male, may indicate ankylosing spondylitis - flex, abduct and externally rotate the hip (“figure of 4”) FINISH by offering to examine the hip joint.