Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
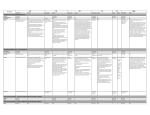
Medicines Q&As Q&A 47.6 Can methylphenidate be used for adults with attention deficit hyperactivity disorder (ADHD)? Prepared by UK Medicines Information (UKMi) pharmacists for NHS healthcare professionals Before using this Q&A, read the disclaimer at www.ukmi.nhs.uk/activities/medicinesQAs/default.asp Date prepared: 11th August 2015 Background ADHD is a behavioural syndrome characterised by the core symptoms of hyperactivity, impulsivity and inattention. Symptoms of ADHD can overlap with symptoms of other related disorders, in adults they include personality disorders, bipolar disorder, obsessive compulsive disorder and substance misuse. (1) ADHD is thought to affect about 3–9% of school-age children and young people in the UK, and about 2-4% of adults worldwide, including the UK, although higher prevalences have been reported in The Netherlands (5%) and France (7.3%). (1-4) Adult ADHD is widely under-recognised. (1, 5) Most young people with a diagnosis of ADHD will go on to have significant difficulties in adulthood, which may include continuing ADHD, personality disorders, emotional and social difficulties, substance misuse, unemployment and involvement in crime. (1) At least 25% of children with ADHD will still have symptoms at the age of 30. (6) Adults may receive a first diagnosis of ADHD having never been diagnosed as a child but have a history of symptoms, or have late onset ADHD, which is considered controversial and relatively rare. (2) ADHD has been diagnosed for the first time in adults aged 55-70 years. (7) A clinical guideline on the diagnosis and management of ADHD in children, young people and adults was issued by the National Institute for Health and Clinical Excellence (NICE) in September 2008 and updated in March 2013. (1) It states that people with ADHD require integrated care that addresses a wide range of personal, social, educational and occupational needs. Care should be provided by adequately trained healthcare and education professionals. Adults presenting with symptoms of ADHD who do not have a childhood diagnosis should be referred for assessment by a mental health specialist trained in the diagnosis and management of ADHD. Adults who have previously been treated for ADHD as children or young people and have symptoms suggestive of continuing ADHD should be referred to adult psychiatric services for assessment. Drug treatment for adults with ADHD should always form part of a comprehensive treatment programme that addresses psychological, behavioural and educational or occupational needs. Drug treatment is first line treatment for adults with ADHD with either moderate or severe levels of psychological, social and/or educational or occupational impairment. (1) Answer The NICE clinical guideline states that following a decision to start drug treatment in adults with ADHD, methylphenidate should normally be tried first. If methylphenidate is ineffective or unacceptable, atomoxetine or dexamfetamine can be tried. (1) There are methylphenidate preparations available in the UK with information on administration to adults in their summary of product characteristics (SPC). Concerta XL, Matoride XL and Medikinet XL (10-60mg) can be used in adolescents whose symptoms persist into adulthood and who have shown clear benefit from treatment, so it may be appropriate to continue treatment into adulthood. However, starting treatment with these preparations in adults is not appropriate. Safety and efficacy have not been established for the initiation of treatment in adults or the routine continuation of treatment beyond 18 years of age. If treatment withdrawal has not been successful when an adolescent has reached 18 years of age continued treatment into adulthood may be necessary. The need for further treatment of these adults should be reviewed regularly and undertaken annually. (8-16) The other methylphenidate preparations currently available in the UK are not licensed for use in adults (17-20). However, methylphenidate hydrochloride is licensed for use in adults in America. (21) Atomoxetine is licensed for use in adults with ADHD in the UK. The presence of pre-existing symptoms in childhood should be confirmed. (22) From the NHS Evidence website www.evidence.nhs.uk 1 Medicines Q&As The NICE guideline development group (GDG) identified a number of studies published between 1976 and 2007 that assessed the efficacy and safety of pharmacological treatments for ADHD. However, a large majority were excluded as they lacked validated outcome measures. (23) The use of methylphenidate in adults is based on the results of 3 studies – see table 1. The NICE GDG summarised that in adults with ADHD, high dose methylphenidate showed evidence of a reduction in ADHD symptoms as rated by an investigator but a small effect of improvement in medium doses as measured from self-reports. There was also evidence of global clinical improvement when compared with placebo. (23) Only one RCT (24) assessed side effects and indicated that high dose methylphenidate is more likely than placebo to cause particular side effects: decreased appetite, gastrointestinal problems, tension, cardiovascular complaints, depression, dizziness, anxiety, autonomic symptoms, increased energy, tics, skin problems, bruising and sexual problems. Methylphenidate may reduce the risk of discontinuation when compared with placebo. Long-term studies of side effects in adults are scarce. Safety reviews have indicated an association between the use of methylphenidate and sudden death, however, given the lack of background rates the evidence is inconclusive. The GDG concluded that methylphenidate is effective in reducing ADHD core symptoms and in producing clinical improvement as rated by investigators in adults with ADHD and high dose methylphenidate may increase side effects. (23) Table 1 - Efficacy results from double blind, placebo controlled studies in adults with ADHD Ref no. 24 25 26 Study details Methylphenidate preparation 36mg SR tablet [osmotic release oral system] Mean daily dose 80.9 31.8mg 146 adults R, DB, PC, PD 6 weeks duration 5mg & 10mg IR capsules 82 ± 22mg 45 adults R, DB, PC, CO 6 weeks duration 10mg IR tablets 149 adults R, DB, PC 6 weeks duration (0.99 ± 0.32 mg/kg) (1.1 ± 0.24 mg/kg) Mean total daily dose not stated (0.91mg/kg, range 0.541.04 mg/kg) Results at study endpoint 66% methylphenidate vs. 39% placebo subjects reported much or very much improved on the CGI Improvement scale and a >30% reduction in ADHD symptoms on AISRS (p<0.001). 68% methylphenidate vs. 17% placebo subjects reported much or very much improved on the CGI Improvement scale and a >30% reduction in ADHD symptoms on AISRS (p<0.0001). 38% methylphenidate vs. 7% placebo subjects had a decrease of at least 2 points on the CGIADHD and a >30% symptom reduction measured by the DSMIV ADHD rating scale (p=0.003). Key: R = randomised, DB = double blind, PC = placebo controlled, CO = cross over, PD = parallel design, SR = sustained release, IR = immediate release, CGI-ADHD = Clinical Global Impression scale for ADHD (investigator assessment), AISRS = Adult ADHD Investigator System Report Scale, DSM-IV ADHD = Diagnostic and Statistical Manual of Mental Disorders 4th edition ADHD rating scale (patient self assessment) A comparison of the acute efficacy and tolerability of the 2 different methylphenidate preparations used in the Biederman et al (24) and Spencer et al (25) studies concluded that once daily doses of SR methylphenidate had similar efficacy to three times daily doses of IR methylphenidate. (27) The NICE GDG reviewed the guideline and decided in February 2014 that it should be updated, particularly because atomoxetine is now licensed for starting treatment in adults with ADHD. (28) A systematic review of 8 meta-analyses assessing pharmacological and psychosocial interventions for adults with ADHD indicates that stimulants (including methylphenidate) are effective in decreasing ADHD symptoms on a short-term basis with a medium to large effect size. Short-acting stimulants might be superior to long-acting stimulants, but no data on difference in adherence are available for the comparison of these 2 types of formulation. (29) From the NHS Evidence website www.evidence.nhs.uk 2 Medicines Q&As A Cochrane systematic review (11 trials, n=474) which evaluated the efficacy and tolerability of IR methylphenidate versus placebo in the treatment of adults with ADHD showed that IR methylphenidate decreased hyperactivity, impulsivity and inattentiveness compared to placebo. Subgroup analysis comparing high versus low doses did not indicate that higher doses of IR methylphenidate were associated with greater efficacy. The trial data suggest that adverse effects from IR methylphenidate for adults with ADHD are not of serious clinical significance. (30) Evidence based guidelines for the pharmacological management of ADHD from the British Association for Psychopharmacology in 2014 recommend use of methylphenidate as a first line stimulant drug. Response to treatment should be assessed in follow up visits using rating scales to objectively check symptoms before and after medication. The clinician should increase the dose until optimal management of symptoms is achieved. If the patient cannot tolerate higher doses or no effect is seen after a trial of adequate duration, a switch to a non-stimulant drug is recommended. (31) Since the NICE clinical guideline publication, a number of papers have reviewed and assessed the efficacy, tolerability and long term use of IR and SR methylphenidate in adults with ADHD. A review of controlled and naturalistic studies demonstrate efficacy for both methylphenidate formulations and indicate that use of methylphenidate results in statistically significant improvement of ADHD symptoms according to various rating scales. (32-34) Quality of life is improved as well. (35) Some adults with ADHD do not have a sufficient response to methylphenidate, to date no reliable neurobiological markers of treatment response have been identified. (36) It has been suggested that ADHD in adults could be split into 2 presenting types- inattentive and emotional dysregulation. Those with emotional dysregulation have a greater severity of symptoms, although both types respond well to methylphenidate. (37) Patients with a greater severity of ADHD have a good response to methylphenidate independent of co-morbidities. (38) A meta-regression analysis of the efficacy of methylphenidate for adults with ADHD showed an improvement in symptoms in a dose dependent fashion. (39) The efficacy of methylphenidate appears to be reduced in patients with comorbid disorders. (33, 39, 40) The studies included in the NICE clinical guideline were only of 6 weeks duration, other studies have been conducted from 24 weeks to more than 4 years. (32, 33) A naturalistic follow up study showed that treatment of ADHD in adults for more than 2 years was associated with better functioning than treatment for 2 years or less. (33) All the studies showed quite high rates of discontinuation of methylphenidate, some over 50%. In many cases, discontinuation was due to adverse effects or lack of efficacy due to the low doses used in the studies. (32, 33) There is a positive correlation between dropout rate and the dose of methylphenidate. (34) Post-hoc analysis of a randomised, double blind, placebo controlled trial with SR methylphenidate 54mg and 72mg suggest that women, newly diagnosed patients, patients with a substance use disorder and subjects with high educational degrees seem to have a higher risk of non-adherence and therefore a reduction in improvement in symptoms. (41) Cardiovascular adverse effects have been noted in the clinical trials, methylphenidate is associated, on average, with only small elevations in blood pressure and heart rate. Increased risk of sudden death or ventricular arrhythmia has not been demonstrated in large population based studies. (32) Summary NICE clinical guidelines on the diagnosis and management of ADHD in children, young people and adults state that following a decision to start drug treatment in adults with ADHD, methylphenidate should normally be tried first. Methylphenidate preparations currently available in the UK are not licensed for use in adults. The SPCs for Concerta XL, Matoride XL and Medikinet XL (10-60mg) say they can be used in adolescents whose symptoms persist into adulthood and who have shown clear benefit from treatment, so it may be appropriate to continue treatment into adulthood. However, starting treatment with Concerta XL, Matoride XL and Medikinet XL in adults is not appropriate. Methylphenidate is effective in reducing ADHD core symptoms and in producing clinical improvement in adults with ADHD when assessed against investigator rating scales. From the NHS Evidence website www.evidence.nhs.uk 3 Medicines Q&As Improvement in symptoms is dose dependent and sustained release and immediate release methylphenidate preparations have similar efficacy in adults. A naturalistic follow up study showed that treatment of ADHD in adults for more than 2 years was associated with better functioning than treatment for 2 years or less. Co-morbidity at baseline is a predicter of poorer outcome. There is a positive correlation between dropout rate and the dose of methylphenidate. Women, newly diagnosed patients, patients with a substance use disorder and subjects with high educational degrees seem to have a higher risk of non-adherence. Methylphenidate is associated, on average, with only small elevations in blood pressure and heart rate. Increased risk of sudden death or ventricular arrhythmia has not been demonstrated in large population based studies. Limitations This question has only examined the use of methylphenidate for treatment of adults with ADHD. Other stimulants have also been studied e.g. dexamphetamine, atomoxetine. Non-stimulants that may provide a response include bupropion, monoamine oxidase inhibitors, lithium and venlafaxine. (2) References 1. NICE Clinical Guideline 72. Attention deficit hyperactivity disorder: diagnosis and management of ADHD in children, young people and adults. Issued September 2008, last modified March 2013. Accessed via http://www.nice.org.uk on 08/07/15. 2. Bazire S. Psychotropic Drug Directory 2014. Lloyd-Reinhold Communications. p34-37 3. McCarthy S, Wilton L et al. The epidemiology of pharmacologically treated attention deficit hyperactivity disorder (ADHD) in children, adolescents and adults in UK primary care. BMC Paediatrics 2012; 12: 78 http://www.biomedcentral.com/1471-2431/12/78 4. Brod M, Pohlman B et al. Comparison of the burden of illness for adults with ADHD across seven countries: a qualitative study. Health and Quality of Life Outcomes 2012; 10: 47 http://www.hqlo.com/content/10/1/47 5. Anon. Adults with ADHD: ignored and under-treated. Drug and Therapeutics Bulletin 2011; 49 (7): 73 6. Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines in Psychiatry, 12 th edition, 2015. Wiley Blackwell. p385-7. 7. Manor I; Rozen S; et al. When does it end? Attention-deficit/hyperactivity disorder in the middle aged and older populations. Clinical Neuropharmacology 2011; 34 (4): 148-54. 8. Summary of Product Characteristics - Concerta XL 18mg prolonged-release tablets. JanssenCilag Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 16/06/15]. 9. Summary of Product Characteristics - Concerta XL 27mg prolonged-release tablets. JanssenCilag Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 16/06/15]. 10. Summary of Product Characteristics - Concerta XL 36mg prolonged-release tablets. JanssenCilag Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 16/06/15]. 11. Summary of Product Characteristics - Concerta XL 54mg prolonged-release tablets. JanssenCilag Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 16/06/15]. 12. Summary of Product Characteristics - Matoride XL 18mg prolonged-release tablets. Sandoz Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 17/02/15]. 13. Summary of Product Characteristics - Matoride XL 36mg prolonged-release tablets. Sandoz Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 06/02/15]. 14. Summary of Product Characteristics - Matoride XL 54mg prolonged-release tablets. Sandoz Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 06/02/15]. 15. Summary of Product Characteristics - Medikinet XL. Flynn Pharma Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 08/11/13]. 16. Summary of Product Characteristics - Medikinet XL 50mg and 60mg Modified Release Capsules Hard. Flynn Pharma Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 17/06/14]. 17. Summary of Product Characteristics - Equasym XL 10mg, 20mg & 30mg capsules. Shire Pharmaceuticals Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 10/03/14]. 18. Summary of Product Characteristics - Ritalin tablets. Novartis Pharmaceuticals UK Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 05/05/15]. From the NHS Evidence website www.evidence.nhs.uk 4 Medicines Q&As 19. Summary of Product Characteristics - Medikinet tablets. Flynn Pharma Ltd. Accessed via http://emc.medicines.org.uk on 08/07/15 [last revised 21/12/11]. 20. Summary of Product Characteristics - Medikinet XL 5mg. Flynn Pharma Ltd. Accessed via http://emc.medicines.org.uk on 07/08/15 [last revised 21/12/11]. 21. DRUGDEX® Drug Evaluation – methylphenidate. DRUGDEX electronic version, Thomson Micromedex, USA. Accessed via http://www.thomsonhc.com on 07/06/13. 22. Summary of Product Characteristics – Strattera 10mg, 18mg, 25mg, 40mg, 60mg, 80mg or 100mg hard capsules. Eli Lilly and Company Ltd. Accessed via http://emc.medicines.org.uk on 02/07/13 [last revised 28/05/13]. 23. National Collaborating Centre for Mental Health. ADHD. Diagnosis and management of ADHD in children, young people and adults. The British Psychological Society and The Royal College of Psychiatrists, 2009. Accessed via http://www.nice.org.uk on 14/07/15. 24. Biederman J, Mick E et al. A randomised, placebo-controlled trial of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder. Biological Psychiatry 2006; 59: 829-35. 25. Spencer T, Biederman J et al. A large, double-blind, randomised clinical trial of methylphenidate in the treatment of adults with attention-deficit/hyperactivity disorder. Biological Psychiatry 2005; 57: 456-63. 26. Kooij JJS, Burger H et al. Efficacy and safety of methylphenidate in 45 adults with attentiondeficit/hyperactivity disorder. A randomised placebo-controlled double-blind cross-over trial. Psychological Medicine 2004; 34: 973-82. 27. Biederman J, Mick EO et al. Comparative acute efficacy and tolerability of OROS and immediate release formulations of methylphenidate in the treatment of adults with attentiondeficit/hyperactivity disorder. BMC Psychiatry 2007; 7: 49. 28. NICE Centre for Clinical Practice – Surveillance Programme. Surveillance review of CG72: ADHD. Recommendation for Guidance Executive. Feb 2015 http://www.nice.org.uk/guidance/cg72/resources/attention-deficit-hyperactivity-disorder-adhdsurveillance-review-decision3 29. Moriyama TS, Polanczyk GV, Terzi FS et al. Psychopharmacology and psychotherapy for the treatment of adults with ADHD-a systematic review of available meta-analyses. [Review]. CNS Spectrums 2013; 18: 296-306. 30. Epstein T, Patsopoulos NA, Weiser M. Immediate-release methylphenidate for attention deficit hyperactivity disorder (ADHD) in adults. Cochrane Database of Systematic Reviews 2014, Issue 9. Art. No.: CD005041. DOI: 10.1002/14651858.CD005041.pub2. 31. Bolea-Alamanac B, Nutt DJ, Adamou M et al. Evidence-based guidelines for the pharmacological management of attention deficit hyperactivity disorder: Update on recommendations from the British Association for Psychopharmacology. Journal of Psychopharmacology 2014; 28: 179-203. http://www.bap.org.uk/pdfs/ADHD_Guidelines.pdf 32. Fredriksen M, Halmoy A, Faraone SV et al. Long-term efficacy and safety of treatment with stimulants and atomoxetine in adult ADHD: A review of controlled and naturalistic studies. European Neuropsychopharmacology 2013; 23: 508-27. 33. Lensing MB, Zeiner P et al. Four year outcome in psychopharmacologically treated adults with attention-deficit/hyperactivity disorder: a questionnaire survey. Journal of Clinical Psychiatry 2013; 74 (1): e87-93 34. Santosh PJ, Sattar S et al. Efficacy and tolerability of pharmacotherapies for attention-deficit hyperactivity disorder in adults. CNS Drugs 2011; 25 (9): 737-63 35. Mattos P, Louza MR, Fernandes Palmini AL et al. A multicentre, open-label trial to evaluate the quality of life in adults with ADHD treated with long-acting methylphenidate (OROS MPH): Concerta quality of life (CONQoL) study. Journal of Attention Disorders 2013; 17 (5): 444-8. 36. Retz W, Retz-Junginger P. Prediction of methylphenidate treatment outcome in adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neurosci 2014; 264 (suppl1): S35-43. 37. Reimherr FW, Marchant BK, Gift TE et al. Types of adult attention-deficit hyperactivity disorder (ADHD): baseline characteristics, initial response, and long-term response to treatment with methylphenidate. Atten Def Hyp Disord 2015; 7: 115-128. 38. Victor MM, Rovaris DL, Salgado CAI et al. Severity but not comorbidities predicts response to methylphenidate in adults with attention-deficit/hyperactivity disorder. Results from a naturalistic study. J Clin Psychopharmacol 2014; 34: 212-7. From the NHS Evidence website www.evidence.nhs.uk 5 Medicines Q&As 39. Castells X, Ramos-Quiroga JA et al. Efficacy of methylphenidate for adults with attention-deficit hyperactivity disorder. A meta-regression analysis. CNS Drugs 2011; 25 (2): 157-69 40. Fredriksen M, Dahl AA, Martinsen EW et al. Effectiveness of one-year pharmacological treatment of adult attention-deficit/hyperactivity disorder (ADHD): An open-label prospective study of time in treatment, dose, side-effects and comorbidity. European Neuropsychopharmacology 2014; 24: 1873-84. 41. Kooji JJS, Rosler M et al. Predictors and impact of non-adherence in adults with attentiondeficit/hyperactivity disorder receiving OROS methylphenidate: results from a randomized, placebo-controlled trial. BMC Psychiatry 2013;13:36 http://www.biomedcentral.com/1471-244X/13/36 Quality Assurance Prepared by Katie Smith, East Anglia Medicines Information Service Date Prepared 11th August 2015 Checked by Sarah Cavanagh, East Anglia Medicines Information Service Date of check 21st August 2015 Search strategy Embase: [[ATTENTION DEFICIT DISORDER/ AND ADULT/] AND METHYLPHENIDATE] [Limit to: Publication Year 2013-2015 and Human and (Human Age Groups Adult 18 to 64 years) and English Language and (Clinical Trials Clinical Trial)] Medline: [ATTENTION DEFICIT DISORDER WITH HYPERACTIVITY/ AND ADULT/] AND METHYLPHENIDATE/ [Limit to: Publication Year 2013-2015 and (Publication Types Clinical Trial, All) and Humans and (Age Groups All Adult 19 plus years) and English Language] In-house database/resources: search terms = methylphenidate, hyperkinetic syndrome, adult Electronic Medicines Compendium: search term = methylphenidate, adults, ADHD NICE Evidence: search terms = methylphenidate + adult + hyperkinetic syndrome DrugDex methylphenidate drug evaluation: ADHD, adults From the NHS Evidence website www.evidence.nhs.uk 6