Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
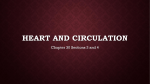
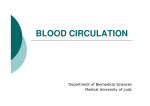
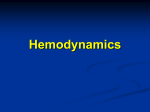
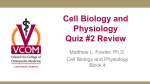
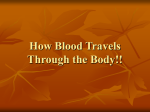
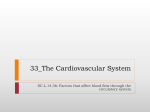
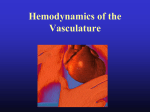
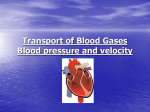
Amir Golnabi ENGS 166 – Spring 2008 Paper #3 – 04/30/08 Hemodynamics and Factors Affecting Blood Flow Blood flow is the amount of blood that flows through any tissue in a given period of time and is usually measured in mL/min. Total blood flow, which is the volume of blood that circulates through the systemic and pulmonary blood vessels each minute is known as cardiac output (CO), and is a function of heart rate and stroke volume. Cardiac output (CO) = heart rate (HR) x stroke volume (SV). There are two factors that determine how the cardiac output is distributed into different body tissues through circulatory system. The first one is the pressure difference of different parts of the body, and the second one is the resistance of specific blood vessels to blood flow. The greater the pressure difference, the greater the blood flow, and the higher the resistance, the smaller the blood flow. My goal in this paper is to describe these two factors in a quantitative manner: Blood Pressure (BP): Blood flows within the circulatory system from regions of high pressure to regions of lower pressure. Contraction of the ventricles generates a hydrostatic pressure which is exerted by blood on the walls of a blood vessel. This pressure is called blood pressure. Normal BP in a young adult at rest rises to about 110 mmHg during ventricular contraction, systole, and drops to about 70 mmHg during ventricular relaxation, diastole. As blood leaves the aorta and flows through the systemic circulation, its pressure falls gradually as it gets farther from the left ventricle. Blood pressure decreases to about 35 mmHg as blood passes from systemic arteries through systemic arterioles and into capillaries, where the oscillations between systolic BP and diastolic BP disappear. When blood reaches de venous end of capillaries, its pressure can be as low as 16 mmHg and continues to drop as blood enters systemic veins. This is due to the fact that these vessels are farthest from the left ventricle. Finally, blood pressure reaches 0 mmHg as blood flows into the right heart. Figure1 shows the BP’s in various parts of the cardiovascular system. 1 Tortora, Gerard, and Bryan Derrickson. Principles of Anatomy and Physiology. Wiley, 2006. 747. Figure1 The mean arterial pressure (MAP) is the average blood pressure in arteries. We should keep in mind that since the arterial pressure is closer to diastolic pressure during the greater portion of the cardiac cycle, MAP is not the average of systolic and diastolic pressure. Indeed, it is roughly one-third of the way between the diastolic and systolic pressures. MAP can be estimated as follows: MAP = diastolic BP + 1/3(systolic BP – diastolic BP) Therefore, in a person with systolic BP of 120 mmHg and diastolic PB of 80 mmHg, MAP is about: (80 + 1/3(120 – 80)) = 93 mmHg. We know that cardiac output is the heart rate times the stroke volume: CO = HR x SV. Another way to calculate cardiac output is to divide mean arterial pressure (MAP) by vascular resistance (R), which is the opposition to blood flow due to friction between blood and the walls of blood vessels: CO = MAP/R. By rearranging the terms of this last equation, we can see that MAP = CO x R. Due to an increase in either stroke volume or heart rate, the cardiac output increases, and if the resistance stays constant, the mean arterial pressure will consequently increase. Blood pressure also depends on the total volume of blood in the cardiovascular system. A cardiovascular system in an adult normally contains about 5 liters of blood in total. If total blood volume decreases modestly, the homeostatic mechanism, that helps maintain blood pressure, can compensate for it; however, if the decrease in blood volume 2 is greater than 10% of the total, blood pressure drops. Conversely, when for any reason, such as water retention in the body, blood volume increases, blood pressure tends to increase as well. The second factor that determines how the cardiac output reaches different body tissues through circulatory system is the resistance. As mentioned earlier, vascular resistance is generated due to friction between blood and the walls of blood vessels and resists to blood flow. Vascular resistance depends on three factors: (1) size of the blood vessels, (2) blood viscosity, and (3) total blood vessels length. Let’s study each of them in more detail: 1. Size of the lumen: The smaller the lumen of a blood vessel, the greater its resistance to blood flow. Resistance and the diameter (d) of the blood vessel’s lumen are inversely proportional and follow the “forth power law”. According to this law, the resistance increases in proportion to the inverse of the forth power of the diameter: R ∝ 1 . For instance, if the d4 diameter of a blood vessel decreases by one-half, its resistance to blood flow increases 16 times. It’s important to notice that even minor changes in the diameter of a vessel can affect significantly its resistance. Narrowing and widening of the vessels resulting from contraction and relaxation of the muscular wall of the vessels are called vasoconstriction and vasodilation, respectively. Due to vasoconstriction and vasodilation of the tissue’s arterioles, there are normally constant fluctuations in blood flow through a given tissue. When arterioles contract, resistance increases and as a result, blood pressure goes up. Conversely, when arterioles dilate, resistance decreases and blood pressure falls. 2. Blood Viscosity: In order to understand the concept of blood viscosity, consider the experiment shown in Figure2. 3 Figure2 A shearing force F is moving the top plate with velocity (v), and the bottom plate is kept in place with velocity zero. This situation is very similar to what happens in main blood vessels: Different layers of the blood move with different velocities. The difference in velocity of different blood layers causes a shearing action (friction) between them. The rate of shear (γ) is the relative displacement of one fluid layer with respect to the next. The rate of shear is the slope of the velocity profile as shown in Figure3, and is calculated as v/h, where v is the velocity of the top layer, and h is the distance between the layers. The units of shear rate are 1/s. Figure3 The required force to gain a certain velocity depends on the contact area (A) between fluid and layers. Blood moves by the action of shear stress, which is defined as the force per area, τ = F/A, with units Pa or Newton/m^2 (N/m^2). Going back to Figure2, if the shear force (shear stress) is measured at different velocities (v) of the top plate, we can plot the shear stress (τ) versus the shear rate (γ) (Figure4). The slope of the relationship between shear stress and shear rate is the viscosity and it can be calculated as: η = shear stress / shear rate = τ / γ Figure4 4 The units of viscosity (η) are Pa.s = Ns/m^2, or Poise (dynes.s/cm^2) Blood consists of two major components: plasma and particles, such as the red blood cells. Hematocrit (Ht) is the percentage of the blood that is cells and not plasma. Therefore, hematocrit of 40 means that 40% of the blood volume is cells and the remainder is plasma. Hematocrit is normally about 46% for men and 38% for women. Thus, the viscosity of blood depends on both the viscosity of the plasma and the hematocrit. Higher hematocrit implies higher blood viscosity. The relationship between blood viscosity and hematocrit can be expressed as: η =ηplasma (1 + 2.5 Ht ) Given that the viscosity of plasma is about 0.015 Poise and hematocrit for men is normally about 46, the viscosity of whole blood can be calculated as follows: η = 0.015(1 + 2.5 ×0.46 ) = 0.032 Poise There are various factors that affect the viscosity of blood. One of them is the velocity of the blood. As the velocity (shear rate) increases, viscosity decreases. However, the blood requires to reach a certain shear stress to flow, the so-called yield stress. The viscosity of blood also depends on the size of the blood vessel. In small blood vessels, and at higher velocities, blood viscosity is lower. Finally, viscosity can vary significantly with changes in temperature. If body temperature decreases just 1ºC, blood viscosity can increase 2%. Accordingly, the blood viscosity in a cold foot is much higher than in the brain. 3. The last factor affecting vascular resistance is the total length of blood vessel. Resistance to blood flow through a vessel is directly proportional to the length of the blood vessel. The reason obese people often have hypertension is that they have additional blood vessels in their adipose tissue, and consequently their total blood vessel length is longer. The longer the blood vessel, the greater the resistance to blood flow, and as a result, their blood pressure is regularly more elevated than normal. For each extra kilogram of fat, an estimated 650 km (about 400 miles) of additional blood vessels can develop in our body! 5 Once we have studied all factors affecting the circulation of blood in the vascular system, we can introduce Poiseuille’s Law to describe the relationship between these factors and calculate the rate of blood flow (F): F = π ∆P r 4 8ηl Where ∆P is the pressure difference between two ends of the vessel, r is the radius of the vessel, η is the blood viscosity, and l is the length of the vessel. As noted earlier, higher difference in blood pressure at both ends of a vessel, in addition to the diameter of the lumen, have a positive relationship with the rate at which blood flows. Conversely, blood viscosity and the length of the vessel are inversely in proportion to the rate of blood flow. 6 References: "An Introduction to Blood Pressure". Maryland Virtual High School of Science and Mathematics. 04/27/2008 <http://mvhs.shodor.org/edgrid/bloodpressure/bptoblt.pdf>. Bipin , Upadhyay. "BLOOD VISCOSITY FUNCTIONAL PARAMETERS". COLLEGE OF BIOMEDICAL ENGINEERING AND APPLIED SCIENCES. 04/28/2008 <http://www.biomedical.edu.np/biomed_files/>. Freeman, Scott. Biological Science. Upper Saddle River, NJ: Pearson Prentice Hall, 2005. Guyton, Arthur, and John Hall. Textbook of Medical Physiology. PA: Elsevier, 2006. Purves, William K.; David Sadava, Gordon H. Orians, H. Craig Heller (2004). Life: The Science of Biology, 7th, Sunderland, Mass: Sinauer Associates, 954. Tortora, Gerard, and Bryan Derrickson. Principles of Anatomy and Physiology. Wiley, 2006. 7