Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
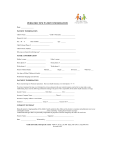
New OB Patient History The Basics: Current Medications: _____________________ Name: ________________________________ _______________________________________ Home phone #:__________________________ _______________________________________ Cell phone #: ___________________________ _______________________________________ Father of the Baby: Education: _______________________________________ □ Husband □ Domestic Partner Last Grade Level Completed: □ High School □ College Years married / together? _________ □ Post Grad Emergency Contact Person: Did you have any special education needs in _______________________________________ school? Relationship to you: How do you learn best? yes _______________________________________ □ Listening / watching Emergency Contact Phone #: □ Demonstration _______________________________________ □ Reading no Background Information: Are you enrolled in any of the following? Your occupation: WIC yes no _______________________________________ Food Stamps yes no Your Job Title: Families First AFDC yes no _______________________________________ Social Security yes no Father of the Baby’s occupation: How many meals do you eat in a day? _______________________________________ Father of the Baby’s Job Title: ___________________ Do you have an advanced directive? _______________________________________ yes no Your Race: Do you want information about an advanced _______________________________________ directive [living will]? Your Country of birth: yes no _______________________________________ Do you have any spiritual or cultural needs that Your primary language spoken: would effect how we care for you? _______________________________________ Your Religion: yes no Explain:________________________________ _______________________________________ _______________________________________ Drug Allergies? _______________________________________ yes no Explain_________________________________ Do you have any objections to receiving blood Are you allergic to latex? yes no products? Food allergies? yes no Pre-pregnancy weight: ____________________ yes no Do you live in a: Do you have a birth plan? yes no □ House GYN History □ Apartment Do you have your menstrual cycle every 28 – 30 □ Other___________________ days? Where you live do you have the following? yes If not, how often? no ___________________ Electricity yes no What was the first day of your last menstrual Water yes no period? ________________________________ Well water yes no How was your pregnancy confirmed? Cooking facilities / kitchen Stairs □ Home pregnancy test yes no yes no What is your current form of transportation? □ Personal vehicle □ Doctor’s office/clinic test Medical History & Health Maintenance Do you exercise regularly? yes no Are your immunizations up to date? □ Family and friends yes □ Public transportation no Do you drink alcoholic beverages? □ TennCare transportation yes no Planning for your baby? Do you use street drugs? yes no Do you have an infant car seat? Do you smoke? yes no yes no How do you want to feed your baby? Past Pregnancies (please use another sheet of paper if you need more room) □ Breast and Bottle Pregnancy # □ Breast only Month/Year of □ Bottle only Birth □ Not sure Male / Female Birth weight If your baby is a boy, do you want him circumcised? yes no Vaginal birth, When you deliver your baby, what type of pain c-section, medication do you want? miscarriage, or abortion □ Epidural Pain □ IV Medicine Management □ None What type of birth control do you want to use after your baby is born? Feeding Breast or Bottle □ Pills Childs Name □ Depo Provera Injections Weeks at time □ IUD of delivery □ Permanent Sterilization Hours in labor □ Unsure Problems? Will your baby be placed for adoption? yes no 1 2 3 4 Medical History and Health Maintenance Patient Family Unsure Multiple Births [i.e. twins] Yes No Yes No Malignancies [i.e. cancer] Yes No Yes No Hypertension [i.e. high blood pressure] Yes No Yes No Heart Disease Yes No Yes No Pulmonary Disease [i.e. asthma] Yes No Yes No GI Problems [i.e. crohn’s disease] Yes No Yes No Breast Disease Yes No Yes No Urinary tract problems [including UTI’s & Yes No Yes No Endocrine/Metabolic [i.e. diabeties/thyroid] Yes No Yes No GYN problems Yes No Yes No Abnormal pap smears Yes No Yes No Fibroids Yes No Yes No Abnormal uterine bleeding Yes No Yes No Incompetent cervix Yes No Yes No Other: ____________ Yes No Yes No Infertility/recurrent miscarriage Yes No Yes No STD’s, HPV, Group B Strep, Herpes Yes No Yes No Phlebitis/varicosities Yes No Yes No Neurological [i.e. seizures] Yes No Yes No Psychiatric [i.e. depression] Yes No Yes No Immunologic/infectious disease Yes No Yes No Operations/ accidents Yes No Yes No Hematologic [i.e. Anemia] Yes No Yes No Other hospitalizations: Yes No Yes No Yes No Yes No Pyelo] [i.e. varicose veins, blood clots] [i.e. Lupus or HIV] _______________________ History of sexual or physical abuse / trauma Genetics: Mother & Father and Your Families History Patient Family Unsure Patient age >34 at delivery Yes No --- --- Thalessemia; MCV < 80 Yes No Yes No Neural Tube Defect Yes No Yes No Congenital Heart Defect Yes No Yes No Down Syndrome Yes No Yes No Jewish, Cajun, French Canadian [tay Yes No Yes No Jewish: Canavan Disease, Gauchers Yes No Yes No Sickle Cell Disease [African American or Yes No Yes No Hemophilia or other blood disorders Yes No Yes No Muscular Dystrophy Yes No Yes No Cystic Fibrosis Yes No Yes No Huntington’s Chorea Yes No Yes No Mental Retardation / Autism [if yes was it Yes No Yes No Other inherited or chromosomal disorder Yes No Yes No Other structural birth defect Yes No Yes No Maternal metabol/endocrine disorders Yes No Yes No Yes No Yes No Yes No Yes No Tobacco, Alcohol, Drugs Yes No Yes No Any other: Yes No Yes No sachs] Caribbean] fragile x? _______] [diabetes, PKU] Patient or baby’s father had a birth defect not listed above: ________________________ Recurrent pregnancy loss [>2] and/or stillbirth ________________________ Vanderbilt Center for Women’s Health – phone 615-343-5700 / fax 615-343-6724 One Hundred Oaks – 719 Thompson Lane, Suite 27100, Nashville TN 37204 Cool Springs – 2009 Mallory Lane, Suite 230, Franklin TN 37067 Clarksville – 647 Dunlop Lane, Suite 206, Clarksville, TN 37040