Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Bronchial Hygiene Therapy (BHT)
Assistant Professor Melissa D. Dearing, BS, RRT-NPS, RCP
Egan's Chapter 40
BHT involves the use of noninvasive airway clearance techniques designed to help
mobilize and remove secretions and improve gas exchange.
BHT involves:
1. CPT - Chest physiotherapy
Can include postural drainage, percussion and vibration
2. CPT can be augmented or replaced by (Description below):
o PEP - Positive Expiratory Pressure
o Flutter Valve - Expiratory Positive Airway Pressure with
Oscillation
o Acapella - Also a PEP device
1
o High Frequency Chest Wall Compression (HFCWC) External Application of oscillation to the chest wall.
o PAP devices - Positive Airway Pressure - used as a
adjunct for airway clearance
Info found at: http://www.regence.com/trgmedpol/dme/dme62.html
Airway Clearance Devices
Description
Pulmonary complications are major causes of morbidity and mortality for patients with compromised
airway clearance mechanisms. Conditions such as high spinal cord injuries, neuro-muscular deficits, or
severe fatigue associated with intrinsic lung disease can diminish the effectiveness of a cough, or
eliminate the ability to cough altogether. Other conditions such as cystic fibrosis, bronchiectasis, and
pneumonia can affect the ability of the lungs to manage secretions and influence the viscosity and
amount of sputum produced. Several adjunctive techniques and devices have been used to assist those
who are otherwise unable to clear pulmonary secretions effectively. (2)
Passive interventions include nebulized bronchodilating medication, postural drainage combined with
chest percussion and/or vibration (P/PD or PDPV), and possibly diaphragmatic (or "quad") coughing
maneuvers. Active interventions consist of autogenic drainage or breathing and coughing techniques
such as forced expiratory technique ("huff" coughing), active cycle breathing (deep breathing or breath
stacking), and pursed lip breathing (creates positive expiratory pressure.) Usually, several of these
mechanisms are utilized in an effective pulmonary toilet program. (3)
Several devices exist that are proposed as an adjunct or alternative to one or more of the mechanisms
described above.
The FLUTTER® mucous clearance device and Acapella™ device are small handheld devices
that provide positive expiratory pressure (PEP.) Exhaling through the device creates
oscillations, or "flutter" in pressures in the airway resulting in loosening of mucous. Other PEP
devices are used with a small volume nebulizer, and function in conjunction with medication
delivery.
2
Mechanical Insufflator-Exsufflator (CoughAssist) is a portable electric device which utilizes a
blower and a valve to alternately apply a positive and then a negative pressure to a patient's
airway in order to assist the patient in clearing retained bronchopulmonary secretions. Air is
delivered to and from the patient via a breathing circuit incorporating a flexible tube, a bacterial
filter and either a facemask, a mouthpiece, or an adapter to a tracheostomy or endotracheal
tube.
Intrapulmonary Percussive Ventilator (IPV) is a type of mechanized chest physical therapy.
Instead of a caretaker clapping or cupping the patient’s chest wall, the IPV device delivers
high-flow jets of air to the airways by a pneumatic flow interrupter at a rate of 100-300
cycles/minute via a mouthpiece. The patient controls variables such as inspiratory time, peak
pressure, and delivery rates.
Intermittent positive pressure breathing (IPPB) devices use pressure to passively fill the lungs
when a breath is initiated. An incorporated manometer and mechanical valves serve to
terminate the flow of inspired air when a predetermined pressure is reached on inhalation. IPPB
breathing circuits are designed to nebulize inhaled medication. Most IPPB devices are powered
by compressed air and are not suitable for home use.
Mechanical percussors are typically electrical devices used in lieu of a caretaker's hands for
chest percussion and/or vibration.
Policy/Criteria
Small hand-held positive expiratory pressure devices, such as the FLUTTER® or Acapella™ devices
may be considered medically necessary as an adjunct to airway clearance in patients who can
demonstrate effective use of the device and when other mechanisms have proven inadequate or
ineffective in mobilizing pulmonary secretions.
Mechanical percussors may be considered medically necessary when the patient or operator of the
powered percussor has received appropriate training by a physician or therapist.
An Insufflator-Exsufflator device, such as the CoughAssist, may be considered medically necessary in
a small subset of patients with neuromuscular disease resulting in an inability to adequately clear their
airways using standard airway clearance mechanisms (as noted in the description above). There should
be evidence of significantly low forced expiratory flow and vital capacity not associated with
obstructive disease.
Intrapulmonary percussive ventilators (i.e., Percussionaire and Percussive Tech HF devices) and
Intermittent Positive Pressure Breathing (IPPB) devices are considered investigational for home use.
Scientific Background
The published literature included a number of small, randomized studies that compared different
mucus clearance techniques, typically in crossover studies. (4,5) Pulmonary function and weight of
expectorated sputum are typically analyzed immediately after treatment. (6) Thus these small shortterm studies focus on intermediate outcomes, and do not include any data regarding long-term
stabilization or improvement of lung function or a decrease in pulmonary exacerbations resulting in
hospitalization. The reliability and validity of sputum weight as a proxy for health outcome is still
unresolved.
The sparse data that are available do not suggest that any one alternative, including the various
oscillatory devices, autogenic drainage, or positive expiratory pressure, is superior to another. The
3
Flutter device, autogenic drainage and positive expiratory pressure are simple devices or maneuvers
that can be learned by most patients.
Mechanical Insufflation-Exsufflation as an Expiratory Muscle Aid
The published data suggest that mechanical insufflation-exsufflation (MI-E) can improve the
intermediate outcome of peak cough expiratory flow. Data regarding its role in the clinical
management of the patient consist of case series (7-13). In some studies, patients have served as their
own control, with a decreased incidence of hospitalization among patients who switch from
tracheostomy to a noninvasive approach, which may include MI-E as one component. While controlled
trials would ideally further delineate who is most likely to benefit from MI-E, particularly those who
would benefit from having a device in the home, such trials are logistically difficult. The
heterogeneous nature of the patients, even among those with similar diseases, almost mandates a case
by case approach for these patients. For example, the clinical utility of MI-E would not only depend on
the physiologic parameters of lung function, but also on the tempo of the disease course, the
availability of home caregivers, and patient preference and motivation. The non-investigational status
for the MI-E device is based on these considerations.
Intrapulmonary Percussive Devices
The clinical data regarding the Percussionaire device are sparse. One early randomized trial of 16
cystic fibrosis patients reported no difference in spirometric measures or number of hospitalizations,
suggesting that the Percussionaire device was equivalent to chest physical therapy. (4) Subsequent
updated literature searches in 2005 and 2006 based on MEDLINE did not return any published clinical
studies that alter the policy conclusions regarding intrapulmonary percussive ventilation devices.
Toussaint and colleagues in a randomized, cross-over study compared assisted mucus clearance
techniques with and without intrapulmonary percussive ventilation (IPV). (14) Eight patients received
five consecutive days of treatment with IPV with nebulization and assisted-clearance techniques and
five days without IPV. At the end of each sequence mucus production was weighed. The mean mucus
production was significantly higher following the sequence with IPV (p=0.01). Marks and colleagues
compared pulmonary function and sputum production following a single treatment with
PercussiveTech HF IPV with changes following a standard chest physiotherapy treatment performed
by a respiratory therapist. There were 10 patients with stable cystic fibrosis in this cross-over study.
Pulmonary function parameters were not significantly different at four hours following either therapy.
There was a slight trend toward more sputum production following the PercussiveTech HF IPV
treatment; however, the difference was not statistically significant. (15) No other studies were found
which address intrapulmonary percussive ventilator devices. The small number of patients and lack of
long term outcomes do not allow conclusions concerning the effectiveness and clinical significance of
IPV on the overall health outcomes of the patient. Therefore, the policy is unchanged.
An updated search of the literature through February 2007 did not return any new clinical trial data that
would alter the policy criteria. Therefore the policy is unchanged.
References
1.
2.
3.
4.
5.
BCBSA Medical Policy Reference Manual, Policy No. 1.01.15
AARC Clinical Practice Guideline, Directed Cough, Use of Positive Airway Pressure Adjuncts to Bronchial Hygiene Therapy. Respir Care
1993;38:495-521
AARC Clinical Practice Guideline, Postural Drainage Therapy. Respir Care 1991;36:1418-1426
Homnick DN, White F, deCastro C. Comparison of effects of an intrapulmonary percussive ventilator to standard aerosol and chest
physiotherapy in treatment of cystic fibrosis. Pediatr Pulmonol 1995;20(1):50–5
Hess DR. The evidence for secretion clearance techniques. Respir Care 2001;46(11):1276-93
4
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Langenderfer B. Alternatives to percussion and postural drainage. A review of mucus clearance therapies: percussion and postural drainage,
autogenic drainage, positive expiratory pressure, flutter valve, intrapulmonary percussive ventilation, and high-frequency chest compression with the
ThAIRapy Vest. J Cardiopulm Rehabil 1998;18(4):283-9
Sivasothy P, Brown L, Smith IE, et al. Effect of manually assisted cough and mechanical insufflation on cough flow of normal subjects,
patients with chronic obstructive pulmonary disease (COPD), and patients with respiratory muscle weakness. Thorax 2001;56(6):438-44
Bach JR. Mechanical insufflation-exsufflation. Comparison of peak expiratory flows with manually assisted and unassisted coughing
techniques. Chest 1993;104(5):1553-62
Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients with neuromuscular disease. Chest 2000;118(5):1390-6
Bach JR, Isikawa Y, Kim H. Prevention of pulmonary morbidity for patients with Duchenne muscular dystrophy. Chest 1997;112(4):1024-8
Bach JR, Niranjan V, Weaver B. Spinal muscular dystrophy type I: a noninvasive respiratory management approach. Chest 2000;117(4):11005
Bach JR, Baird JS, Plosky D et al. Spinal muscular dystrophy type I: management outcomes. Pediatric Pulmonology 2002;34(1):16-22
Bach JR, Wang TG. Noninvasive long-term ventilatory support for individuals with spinal muscular atrophy and functional bulbar musculature.
Arch Phys Med Rehab 1995;76(3):213-7
Toussaint M, De Win H, Steens M et al. Effect of intrapulmonary percussive ventilation on mucus clearance in Duchenne muscular dystrophy
patients: a preliminary report. Respir Care 2003;48(10):940-7
Marks JH, Hare KL, Saunders RA et al. Pulmonary function and sputum production in patients with cystic fibrosis. A Pilot study comparing
the PercussiveTech HF device and standard chest physiotherapy. Chest 2004;125(4):1507-1511
3. BHT also includes a directed cough following CPT and/or the use of
devices listed above.
Normal Airway Clearance
Normal airway clearance requires a patent airway, a functional mucociliary escalator, and an effective
cough.
The mucociliary escalator works form the larynx to the resp. bronchioles.
Mucus originates from the goblet cells and submucosal glands
The wavelike action of the ciliated epithelial cells move the mucus upward
toward the trachea and larynx where it can be expectorated or swallowed.
The cough compliments this escalator by removing foreign material from the
larger airways.
The cough is one of our most important protective reflexes - it keeps our airways
patent.
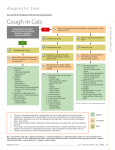
4 Phases of Effective Cough - Fig. 40-1
1. Irritation - an abnormal stimulus (inflammatory, mechanical, chemical or thermal) provokes
sensory fibers to send impulses to the brain's medullary cough center.
2. Inspiration - deep inspiration is initiated (about 1 to 2 Liters in an adult)
3. Compression - Glottic closure and contraction of the expiratory muscles
4. Expulsion - glottis opens, pressure gradient and contraction of expiratory muscles causes
violent expulsion of air from lungs (as high as 500 miles per hour). This displaces mucus
5
and foreign material from the lower airways to the upper airway to be swallowed or
expelled.
Abnormal Airway Clearance
Retention of secretions can be caused by;
altered airway patency
poor mucociliary function
poor cough reflex
Full or partial obstruction can result from retained secretions.
Full obstruction is called mucus plugging - causes atelectasis and impaired oxygenation
Partial obstruction reduces airflow and increases the WOB. This leads to air trapping, over
distension of the lungs and V/Q (ventilation / perfusion) imbalances.
In the top 2 - ventilation is > perfusion created alveolar
deadspace. This is called "a high V/Q."
The bottom 2 represent a "low V/Q." This happens when
ventilation is < perfusion. In this case blood will leave the lungs
with an abnormally low O2 content.
V/Q of 0 represents an anatomical shunt - there is blood flow but
no ventilation. This could be caused by conditions such as
pulmonary edema, pneumonia and atelectasis.
6
ROT: To differentiate between hypoxemia caused by a V/Q imbalance and one caused by shunting
use the 50/50 rule: If Oxygen concentration is more than 50% and the PaO2 is less than 50
mmHg, significant shunting is occurring; otherwise it is a simple V/Q imbalance.
Shunting corrected by CPAP or BiPAP
V/Q imbalance usually corrected by administering O2.
Retained secretions can lead to infection. Infection leads to inflammation thus causing chemical
mediators (leukotrienes, proteases and elastases) to release damaging the airway tissue. This
increases mucus production resulting in a vicious cycle of more infection, more inflammation.....
These problems worsen if the pt. has a poor cough reflex.
How does the ETT cause airway clearance issues?
1. The tube itself causes mucus production.
2. The tube cuff blocks the mucociliary escalator.
3. Movement of the tube and cuff cause erosion of the airway tissue.
4. ETT prevents closure of the glottis impairing the compression phase of cough.
5. Even ETT suctioning can cause damage to the mucosa.
6. Read Box 37-1
Diseases that cause Abnormal Airway Clearance:
A. Internal Obstructions
1.
2.
3.
4.
5.
6.
Foreign Bodies
Tumors
Congenital or acquired thoracic abnormalities (i.e. kyphoscoliosis)
Asthma
Chronic bronchitis
Acute infection
B. Diseases that cause abnormal mucociliary clearance
1. CF - due to abnormal sodium and chloride transport
increase mucus viscosity.
2. Ciliary dysfunction
C. Any condition that affects any of the 4 phases
1. Most common are musculoskeletal and neurological disorders
muscular dystrophy
spinal muscular atrophy
ALS
myasthenia gravis
polio
cerebral palsy
7
Goals and Indications of BHT
The goal of BHT is to mobilize and remove retained secretions thus improving gas exchange and
decrease the WOB.
Indications for BHT- box 40-2
1. Treat an acute condition
copious secretions
acute resp. failure with retained secretions
acute lobar atelectasis
V/Q abnormalities caused by unilateral lung disease
2. Treat Chronic Conditions with Copious Secretions
CF
Bronchiectasis
Ciliary dyskinetic syndromes
Chronic bronchitis
3. Prevention of Retained Secretions
Acute Disease
Immobile pts?
Post op pts?
Exacerbations of COPD?
Chronic Disease
CF
Neuromuscular Disorder
Determining the Need for BHT
See Box 40-3
1.
2.
3.
4.
5.
record review
patient interview
physical assessment
PFT
CXR
8
Methods of BHT
1. Postural Drainage Therapy
A. Turning - rotation of the body around the longitudal axis. Pt should be
turned every 2 hours (Q2) from one side to the other and supported with
pillows. Extreme version of this is to place the pt. prone.
Promotes lung expansion
Improves oxygenation
prevents retention of secretion
Only 2 absolute contraindications: unstable spinal cord injury and arm traction.
There are special rotation beds for pts. who cannot tolerate being turned. These beds rotate on a
schedule (set by RN) usually every 3-4 minutes.
Relative Contraindications include: sever diarrhea, agitation, ICP ↑, drop in BP ↑ 10%, worsening
dyspnea, worsening hypoxia, increase in cardiac arrhythmias.
Additional complications include: vent. disconnect, accidental extubation, accidental aspiration of
vent condensate, and disconnection of IV's or urinary catheters.
Dependent Positioning- refers to placing the "good lung"
down or in the gravity dependent position to help improve gas
exchange within the lung. This improves oxygenation.
o opposite occurs if the good lung is placed superior
o a possible hazard is contamination of the good lung by
drainage from the bad one.
o This is usually a nursing protocol.
B. Postural Drainage - "involves the use of gravity to drain secretions
from the distal lung lobes or segments into the central airways "for
removal via cough or suctioning. There are 12 patient positions for
drainage of segments.
Read AARC Guidelines on page 926 and 927
held for 3 - 15 minutes
position and time may be modified per tolerance of pt.
repeated every 4-6 hours
pts. have to be hydrated to move secretions!!
9
wait 1.5 to 2 hours after eating to avoid reflux and aspiration
coordinate treatment to post pain med.
confirm pt. comfort (hips and shoulders)
Closely monitor pt. with as many parameters as possible
avoid strenuous coughing when pts. head is down (↑ ICP)
If adverse effect occurs, STOP trx immediately and
return pt to normal position. Chart trx. reaction and
inform RN.
Sometimes it is necessary to give critically pts. ↑ O2 due to
the increase in oxygen consumption during the procedure.
Review Complications of Postural Drainage in Table 40-2
Outcome of BHT:
1. Pts have to be optimally hydrated for at least 24 hours to see increased
sputum production.
You can give a bland aerosol with an unheated jet nebulizer
to move retained secretions with inadequately hydrated pts.
CAREFUL, this may cause bronchospasm!
BS may seem to worsen post therapy due to mobilization of
secretions.
Physicians order should be reviewed every: 48 hours for
critical pts, 3 days for non critical and 3 months for home pts.
2. Documentation should include:
position of therapy
time in position
tolerance
amount, color and consistency of sputum
any adverse reactions to therapy
C. Percussion and Vibration 1. Percussion - helps jar retained secretions loose from the
tracheobronchial tree so they can be removed by coughing or suction.
performed during I and E.
2. Vibration - helps mobilize secretions within small airways to the central
airways.
performed only during E.
3. They are used in conjunction with postural drainage.
4. Cupped hands, pneumatic device, silicon cup or electrically powered
device may be used.
10
Electric Powered Percussor
Most units provide frequencies up to 20 to 30 cycles per second. Potential problems include: noise,
excess force and mechanical failure. Electrical devices also pose a potential shock hazard.
Advantages of these devices are: they do not tire and deliver consistent rates, rhythm, and impact.
Manual Percussion
Apply percussion over the segment of lung that needs trx. It is performed with the hands cupped, and
the fingers and thumb are closed. This position traps air between the hand and chest wall as a cushion.
It can be performed on bare skin or a thin gown or bed sheet (preferred). Arms should be outreached
with elbows flexed and wrists loose so that you may rhythmically strike the chest wall in a waving
motion. Percussion should be performed in a circular pattern over the area for a period of 3 to 5
minutes. Avoid tender regions such as sites of surgery or bony areas.
11
Chest Vibration
Vibration is used with percussion. Only perform vibration during "E". Lay one hand on top of the
affected area and place the other hand on top of that one. After the pt. takes a deep breath, exert slight
pressure on the area and initiate a rapid vibration of the hands through the entire "E" cycle.
Coughing and Related Expulsion Techniques
Coughing is an essential component of all BHT. Read ROT on page 932.
A. Directed Cough - is a deliberate maneuver that is taught, supervised, and monitored.
helps compensate for physical limitations to coughing
not effective BHT for pts who don't produce sputum
most effective in clearing secretions from the central, but not peripheral
airways
Technique:
o not possible with paralyzed, obtunded or uncooperative pts.
o Pts must be hydrated
o Pt. should be in a sitting position
o Head and spine should be slightly flexed
o Provide support for the feet to allow for abdominal and thoracic
support
o Breathing control measures are useful for making a more
effective cough
Have pt. breath in slowly and deeply through the nose
with the use of their diaphragm.
Have the pt. bear down against the glottis such as occurs
during straining in the bathroom.
Have the pt. then "stage" their expiratory outbursts in 3
or 4 short bursts.
12
Preoperative training ensures better cooperation and technique post
surgery
In a COPD pt a moderate breath is more effective than a full breath due to
the high pleural pressures in these pts. Too deep of a breath may actually
collapse the smaller airways.
o Have the pt. exhale through pursed lips while bending forward.
This helps increase airflow by displacement of the abdomen.
Neuromuscular pts. may need a Manually assisted cough. While pt. is
exhaling, place pressure on the epigastrium. This maneuver increases the
velocity of the air and may help displace secretions for suctioning.
o This technique (MAC) is contraindicated for the following pts:
osteoporosis
flail chest
unconscious pts with unprotected airways
pregnant women
pts with acute abdominal issues
abdominal aortic aneurysm
hiatal hernia
Review the AARC Guidelines on page 933
B. Forced Expiratory Technique - (Also called the Huff Cough)- is a directed cough
consisting of 1-2 forced expirations of middle to low lung volumes without the closure of
the glottis. This is followed by a period of diaphragmatic breathing and relaxation.
helps to avoid small airway collapse with COPD pts
more effective than directed cough when combined with postural drain.
Not for use with intubated pts. due to their inability to achieve high airflow
through an ETT.
Instructions from USA TODAY:
Huff coughing: Do a huff cough if you feel mucus moving.
1. Take a really deep breath.
2. Use your stomach muscles to make a series of three rapid
exhalations with the airway open, making a "Ha, ha, ha" sound.
3. Follow with controlled diaphragmatic breathing.
4. Spit out the mucus.
video on diaphragmatic breathing:
http://www.youtube.com/results?search_type=&search_query=Living+With
+COPD+Part4+Relaxing+With+Diaphragmatic+Breathing&aq=f
The Huff technique helps to avoid small airway collapse (COPD) that occurs
with elevated pleural pressures of strenuous coughing.
C. Active Cycle of Breathing - consists of repeated cycles of breathing control, thoracic
13
expansion and the Forced Expiratory Technique (FET).
Breathing Control consists of diaphragmatic breathing of normal Vt with
relaxation of the upper chest and shoulders.
Thoracic expansion involves deep inhalation with relaxed exhalation. This
will loosen secretions.
FET follows
SEE BOX 40-4 ON PAGE 936
D. Autogenic Drainage (AD) - a modified directed cough where a sitting patient performs
diaphragmatic breathing in 3 stages of various lung volumes. Patients are encouraged to reduce
expiratory flows and create a mucus rattle while suppressing the cough reflex until all 3 phases
are completed.
Spirogram of lung volumes during three phases of autogenic drainage.
Phase I involves a deep inspiratory breath followed by breathing at low lung volumes.
Phase II "unsticks" mucus by breathing at low lung volumes in order to collect mucus in
the middle airways.
Phase III is the "evacuation phase" used to expel mucus from the larger airways. This
phase involves breathing deeper with each breath followed by a cough.
E. Mechanical Insufflation - Exsufflation - "artificial cough machine" - This machine is
used on pts with neuromuscular disorders.
14
This MIE offers:
positive pressure breath of 30 to 50 cmH2O over 1 - 3 seconds via an oral/nasal
mask or tracheal airway.
The airway pressure is then abruptly changed to -30 to -50 cmH2O and maintained
for 2 to 3 seconds.
Peak expiratory flows obtained with this device are in the normal range of about
7.5L/sec
MIE does not promote airway collapse
If applying to trach - the trach cuff must be inflated
If using a mask an abdominal thrust must be timed to the exsufflation period.
A typical MIE trx consists of 5 cycles followed by a period of spontaneous or
supported breathing.
This entire process is repeated 5 times
F. PAP Adjuncts - positive airway pressure- used to mobilize secretions and trx atelectasis.
Never used alone - always with directed cough or other technique
PEP - involves active expiration against a flow resistor
o moves secretions into larger airways
o Followed by a huff or FET maneuver helps to expel mucus
o Provides increased lung function and decreased hyperinflation with
continued use (CF patients).
o Not used in kids ↓ 3 years of age
o Not useful in lung clearance with chronic bronchitis.
o If used with nebulizer trx, bronchodilator administration is better due to
better distribution to the peripheral airways.
G. High Frequency Chest Wall Oscillation Uses a variable air pulse generator and a nonstretch inflatable vest
Air movement creates an oscillatory motion against the pts chest between 5 and 25
Hz.
Sessions are usually 30 minutes long and given between 1 and 6 X per day.
Expensive!
15
H. Flutter Valve - combination of EPAP with high frequency oscillation
oscillation refers to movement of small volumes of air back and forth in the
respiratory tract
A BHT device that consists of a pipe - shaped device with a heavy steel ball sitting
in a "bowl"
This bowl is covered by a perforated cap
Upon exhalation the ball creates a positive expiratory pressure of 10 - 25 cmH2O.
At the same time, the pipe angel causes the ball to flutter back and forth at about 15
Hz.
small and portable; easy to clean and maintain
I. Acapella - A BHT device that looks like a small football. It has a mouthpiece on one end
and a retard outflow adjustment on its opposite end. EPAP is pulsed via an internal lever
that obstructs expiratory flow.
J. Intrapulmonary Percussive Ventilation - (IPV) - uses a pneumatic device to deliver a
series of pressurized gas minibursts at rates of 100 to 225 cycles per minute.
Can be used with a mouthpiece or a mask
Delivers PAP to pt.
trx lasts about 20 minutes
an inline nebulizer can be used to deliver a concurrent bronchodilator trx
Can be used on an intubated pt when attached to the ETT
K. Mobilization and Exercise immobility contributes to retention of secretions
mobilization and frequent position changes are standard preventative measures
for atelectasis and postop pneumonia
improves aeration of the lungs and V/Q matching
adding exercise and coughing to a pts regimen will enhance mucus clearance
o Pts with sever lung disease must have and exercise evaluation done prior
to exercise therapy
Selection of a BHT -
See Box 40-6 - Factors in Selecting BHT
READ TABLE 40-3 RECOMMENDATIONS FOR BHT IN SPECIFIC COND.
EXAMPLE OF BHT PROTOCAL PAGE 942
READ KEY POINTS ON PAGE 943
16
*
*
*
*
a DIRECTED COUGH is just a requested cough with glottic closure
an FET is just a huff (glottis open) and is not a cough
an ACB is diaphragmatic breathing followed by a huff
AD is a series of 3 increased phases of diaphragmatic breathing followed by an FET
17