Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
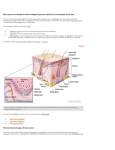
1 Skin cancer Skin cancer is a malignant growth on the skin which can have many causes. Skin cancer generally develops in the epidermis (the outermost layer of skin), so a tumor is usually clearly visible. This makes most skin cancers detectable in the early stages. There are three common types of skin cancer, each of which is named after the type of skin cell from which it arises. Cancers caused by UV exposure may be prevented by avoiding exposure to sunlight or other UV sources, and wearing sun-protective clothes. The use of sunscreen had been recommended in the past, but there is an increasing body of evidence that sunscreen is not entirely safe. Skin cancer is an increasingly common condition. This is in part attributed to increased exposure to ultraviolet radiation, which in turn is thought to be caused by the increased popularity of sun tanning (sun bathing). Lighter-skinned individuals are more vulnerable. In the United States, about one out of every three new cancers arises from the skin. Skin cancers are the fastest growing type of cancer in the United States. Skin cancer represents the most commonly diagnosed malignancy, surpassing lung, breast, colorectal and prostate cancer. More than 1 million Americans will be diagnosed with skin cancer in 2007. Causes Our skin consists of three layers — the epidermis, dermis and subcutis. The epidermis, the topmost layer, is as thin as a pencil line. It provides a protective layer of skin cells that our body continually sheds. Squamous cells lie just below the outer surface. Basal cells, which produce new skin cells, are at the bottom of the epidermis. The epidermis also contains cells called melanocytes, which produce melanin — the pigment that gives skin its normal color. When you're in the sun, these cells produce more melanin, which helps protect the deeper layers of skin. The extra melanin is what produces the darker color of tanned skin. Normally, skin cells within the epidermis develop in a controlled and orderly way. In general, healthy new cells push older cells toward the skin's surface, where they die and eventually are sloughed off. This process is controlled by DNA — the genetic material that contains the instructions for every chemical process in our body. But when DNA is damaged, changes occur in these instructions. One result is that new cells may begin to grow out of control and eventually form a mass of cancer cells. The role of UV light Much of the damage to DNA in skin cells results from ultraviolet (UV) radiation found in sunlight and in commercial tanning lamps and tanning beds. UV light is divided into three wavelength bands: ultraviolet A (UVA), ultraviolet B (UVB) and ultraviolet C (UVC). Only UVA and UVB rays reach the earth. UVC radiation is completely absorbed by atmospheric ozone. At one time scientists believed that only UVB rays played a role in the formation of skin cancer. And UVB light does cause harmful changes in skin cell DNA, including the development of oncogenes — a type of gene that can turn a normal cell into a malignant one. UVB rays are responsible for sunburn and for many basal cell and squamous cell cancers. But UVA also contributes to skin cancer. It penetrates the skin more deeply than UVB does, weakens the skin's immune system and increases the risk of cancer, especially melanoma. Tanning beds deliver high doses of UVA, which makes them especially dangerous. What's more, occasional exposure to intense UVA puts you at greater risk of skin cancer than spending long hours in the sun does. An initial high dose of UV radiation will severely 2 damage melanocytes, but not destroy them. When these damaged cells are subjected to further intense bouts of UVA light, they have little capacity to repair their DNA. This makes them more likely to become malignant. The BCC and the SCC often carry a UV-signature mutation indicating that these cancers are caused by UV-B radiation via the direct DNA damage. However the malignant melanoma is predominantly caused by UV-A radiation via the indirect DNA damage. [2] The indirect DNA damage is caused by free radicals and reactive oxygen species. It has been shown, that the absorption of sunscreen into the skin leads to an increase of free radicals in the skin. [3] Other factors that may contribute to skin cancer Sun exposure doesn't explain melanomas or other skin cancers that develop on skin not ordinarily exposed to sunlight. Heredity may play a role. Skin cancer can also develop from exposure to toxic chemicals or as a result of radiation treatments. Risk factors Skin cancer is most closely associated with chronic inflammation of the skin. This includes: 1. Overexposure to UV-radiation can cause skin cancer either via the direct− or via the indirect DNA damage mechanism. UVA & UVB have both been implicated in causing DNA damage resulting in cancer. Sun exposure between 10AM and 4PM is most intense and therefore most harmful. Natural (sun) & artificial UV exposure (tanning salons) are associated with skin cancer. Since sunbeds cause mostly indirect DNA damage (free radicals) their use is associated with the deadliest form of skin cancer the malignant melanom. 2. Chronic non-healing wounds, especially burns. These are called Marjolin's ulcers based on their appearance and can develop into squamous cell carcinoma. 3. Genetic predisposition, including "Congenital Melanocytic Nevi Syndrome". CMNS is characterized by the presence of "nevi" or moles of varying size that either appear at or within 6 months of birth. Nevi larger than 20 mm (3/4") in size are at higher risk for becoming cancerous. Skin can be protected by avoiding sunlight entirely, or wearing protective clothing while outdoors. Skin cancer is usually caused by exposing skin to UV rays excessively. Reduction of risk Although it is impossible to completely eliminate the possibility of skin cancer, the risk of developing such a cancer can be reduced significantly with the following steps: reducing exposure to ultraviolet (UV) radiation, especially in early years avoiding sunburns ( It was shown that sunscreen - while preventing the sunburn - does not protect from melanoma. [5]) avoiding sun exposure during the day (usually from 10 AM to 3 PM), when the sun is highest in the sky wearing protective clothing (long sleeves and hats) when outdoors using a broad-spectrum sunscreen that blocks both UVA and UVB radiation. Pathology Squamous cell carcinoma is a malignant epithelial tumor which originates in epidermis, squamous mucosa or areas of squamous metaplasia. Macroscopically, the tumor is often elevated, fungating, or may be ulcerated with irregular borders. Microscopically, tumor cells destroy the basement membrane and form sheets or 3 compact masses which invade the subjacent connective tissue (dermis). In well differentiated carcinomas, tumor cells are pleomorphic/atypical, but resembling normal keratinocytes from prickle layer (large, polygonal, with abundant eosinophilic (pink) cytoplasm and central nucleus). Their disposal tends to be similar to that of normal epidermis: immature/basal cells at the periphery, becoming more mature to the centre of the tumor masses. Tumor cells transform into keratinized squamous cells and form round nodules with concentric, laminated layers, called "cell nests" or "epithelial/keratinous pearls". The surrounding stroma is reduced and contains inflammatory infiltrate (lymphocytes). Poorly differentiated squamous carcinomas contain more pleomorphic cells and no keratinization.[6] Types The most common types of skin cancer are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) which may be locally disfiguring but are unlikely to metastasize (spread to other parts of the body). The others, less common types of skin cancer include: Kaposi's sarcoma. This rare form of skin cancer develops in the skin's blood vessels and causes red or purple patches on the skin or mucous membranes. Like melanoma, it's a serious form of skin cancer. It's mainly seen in people with weakened immune systems, such as people with AIDS and people taking medications that suppress their natural immunity, such as people who've undergone organ transplants. Merkel cell carcinoma. In this rare cancer, firm, shiny nodules occur on or just beneath the skin and in hair follicles. The nodules may be red, pink or blue and can vary in size from a quarter of an inch to more than 2 inches. Merkel cell carcinoma is usually found on sun-exposed areas on the head, neck, arms and legs. Unlike basal and squamous cell carcinomas, Merkel cell carcinoma grows rapidly and often spreads to other parts of the body. Sebaceous gland carcinoma. This uncommon and aggressive cancer originates in the oil glands in the skin. Sebaceous gland carcinomas — which usually appear as hard, painless nodules — can develop anywhere, but most occur on the eyelid, where they're frequently mistaken for benign conditions. Precancerous skin lesions. Having less pigment (melanin) in your skin provides less protection from damaging UV radiation. If you have blond or red hair, light-colored eyes, and you freckle or sunburn easily, you're much more likely to develop skin cancer than a person with darker features is. If you developed skin cancer once, you're at risk of developing it again. Even basal cell and squamous cell carcinomas that have been successfully removed can recur in the same spot, often within two to three years. . The risk of developing skin cancer increases with age, primarily because many skin cancers develop slowly. The damage that occurs during childhood or adolescence may not become apparent until middle age. Still, skin cancer isn't limited to older people. Basal cell and squamous cell carcinomas are increasing fastest among women younger than 40. Having skin lesions known as actinic keratoses can increase your risk of developing skin cancer. These precancerous skin growths typically appear as rough, scaly patches 4 that range in color from brown to dark pink. They're most common on the face, lower arms and hands of fair-skinned people whose skin has been damaged by the sun. People with weakened immune systems are at greater risk of developing skin cancer. This includes people living with HIV/AIDS or leukemia and those taking immunosuppressant drugs after an organ transplant. Fragile skin. Skin that has been burned, injured or weakened by treatments for other skin conditions is more susceptible to sun damage and skin cancer. Certain psoriasis treatments and eczema creams might increase your risk of skin cancer. Exposure to environmental hazards. Exposure to environmental chemicals, including some herbicides, increases your risk of skin cancer. Signs and symptoms There are a variety of different skin cancer symptoms. These include crabs or changes in the skin that do not heal , ulcers in the skin. Skin cancer develops primarily on areas of sun-exposed skin, including the scalp, face, lips, ears, neck, chest, arms and hands, and on the legs in women. But it also can form on areas that rarely see the light of day — the palms, spaces between the toes and the genital area. A cancerous skin lesion can appear suddenly or develop slowly. Its appearance depends on the type of cancer. Basal cell carcinoma usually looks like a raised, smooth, pearly bump on the sun-exposed skin of the head, neck or shoulders. Sometimes small blood vessels can be seen within the tumor. Crusting and bleeding in the center of the tumor frequently develops. It is often mistaken for a sore that does not heal. This is the most common skin cancer, accounting for nearly 90 percent of all cases. It's also the most easily treated and the least likely to spread. Basal cell carcinoma usually appears as one of the following: A pearly or waxy bump on your face, ears or neck A flat, flesh-colored or brown scar-like lesion on your chest or back. Squamous cell carcinoma is commonly a red, scaling, thickened patch on sun-exposed skin. Ulceration and bleeding may occur. When SCC is not treated, it may develop into a large mass. Squamous cell carcinoma is easily treated if detected early, but it's slightly more apt to spread than is basal cell carcinoma. Most often, squamous cell carcinoma appears as one of the following: A firm, red nodule on your face, lips, ears, neck, hands or arms A flat lesion with a scaly, crusted surface on your face, ears, neck, hands or arms. Skin cancer is generally divided into two stages: Local. In this stage, cancer affects only the skin. Metastatic. At this point, cancer has spread beyond the skin. Lab Studies: No laboratory studies for skin cancer are available. Imaging Studies: No imaging studies are available for early diagnosis of skin cancer. Current imaging techniques (eg, ultrasound, CT scan, MRI, scintigraphy) may help to detect the rare metastases. Procedures: To diagnose skin cancer, perform a skin biopsy of the affected area and the surrounding healthy tissue. This procedure often is curative. 5 Staging: BCC rarely metastasizes and usually is not staged, unless the cancer is very large and is suspected of spreading to other parts of the body. BCC staging may be similar to the staging of squamous cell carcinoma, according to the following scheme: Stage 0: Cancer involves only the epidermis and has not spread to the dermis. Stage I: Cancer is not large (ie, <2 cm) and has not spread to the lymph nodes or other organs. Stage II: The cancer is large (ie, >2 cm) but has not spread to lymph nodes or other organs. Stage III: The cancer has spread to tissues beneath the skin (eg, muscle, bone, cartilage), and/or has spread to regional lymph nodes, but has not spread to other organs. Stage IV: The cancer can be any size and has spread to other organs. Treatment Most skin cancers can be treated by removal of the lesion, making sure that the edges (margins) are free of the tumor cells. These excisions provide the best cure for both early and high-risk disease. For low-risk disease, radiation therapy and cryotherapy (freezing the cancer off) can provide adequate control of the disease; both, however, have lower overall cure rates than surgery. Treatment for skin cancer and the precancerous skin lesions known as actinic keratoses varies, depending on the size, type, depth and location of the lesions. Often the abnormal cells are surgically removed or destroyed with topical medications. Most treatments require only a local anesthetic and can be done in an outpatient setting. Sometimes no treatment is necessary beyond an initial biopsy that removes the entire growth. If additional treatment is needed, options may include: Freezing. Your doctor may destroy actinic keratoses and some small, early skin cancers by freezing them with liquid nitrogen (cryosurgery). The dead tissue sloughs off when it thaws. The treatment may leave a small, white scar. You may also need a repeat treatment to remove the growth completely. Excisional surgery. This type of treatment may be appropriate for any type of skin cancer. Your doctor cuts out (excises) the cancerous tissue and a surrounding margin of healthy skin. A wide excision — removing extra normal skin around the tumor — may be recommended in some cases. To minimize or avoid scarring, especially on your face, you may need to consult a doctor skilled in skin reconstruction. Laser therapy. A precise, intense beam of light vaporizes growths, generally with little damage to surrounding tissue and with minimal bleeding, swelling and scarring. A doctor may use this therapy to treat superficial skin cancers or precancerous growths on lips. Mohs' surgery. This procedure is for larger, recurring or difficult-to-treat skin cancers, which may include both basal and squamous cell carcinomas. Your doctor removes the skin growth layer by layer, examining each layer under the microscope, until no abnormal cells remain. This procedure allows cancerous cells to be removed without taking an excessive amount of surrounding healthy skin. Because it requires special skill, the surgery should be done only by specially trained doctors. Curettage and electrodesiccation. After removing most of a growth, your doctor scrapes away layers of cancer cells using a circular blade (curet). An electric needle 6 destroys any remaining cancer cells. This simple, quick procedure is common in treating small or thin basal cell cancers. It leaves a small, flat, white scar. Radiation therapy. Radiation may destroy basal and squamous cell carcinomas if surgery isn't an option. Chemotherapy. In chemotherapy, drugs are used to kill cancer cells. For cancers limited to the top layer of skin, creams or lotions containing anti-cancer agents may be applied directly to the skin. Topical drugs can cause severe inflammation and leave scars. Other types of chemotherapy can be used to treat skin cancers that have spread to other parts of the body. Treatments for skin cancer under study include: Photodynamic therapy. This treatment destroys skin cancer cells with a combination of laser light and drugs that makes cancer cells sensitive to light. Photodynamic therapy for precancerous skin lesions is currently available by prescription. Biological therapy (also called immunotherapy). Interferon and interleukin-2 are under study to treat melanoma and nonmelanoma skin cancers. These immunotherapy drugs stimulate your immune system to fight the cancer. Other medications applied to your skin, such as imiquimod (Aldara), enhance your immune reaction to the presence of skin cancer. In the case of disease that has spread (metastasized) further surgical or chemotherapy may be required. References 1. Ackerman AB, Gottlieb GJ: Fibroepithelial tumor of pinkus is trichoblastic (Basalcell) carcinoma. Am J Dermatopathol 2005 Apr; 27(2): 155-9[Medline]. 2. Bowen AR, LeBoit PE: Fibroepithelioma of pinkus is a fenestrated trichoblastoma. Am J Dermatopathol 2005 Apr; 27(2): 149-54[Medline]. 3. Bruce AJ, Brodland DG: Overview of skin cancer detection and prevention for the primary care physician. Mayo Clin Proc 2000 May; 75(5): 491-500[Medline]. 4. Cabrera HN, Cuda G, Lopez M, Costa JA: [Basal cell epithelioma of the vulva in chronic endemic regional arsenic poisoning]. Med Cutan Ibero Lat Am 1984; 12(2): 81-5[Medline]. 5. Cabrera HN, Gomez ML: Skin cancer induced by arsenic in the water. J Cutan Med Surg 2003 Mar-Apr; 7(2): 106-11[Medline]. 6. Cohen MM Jr: Nevoid basal cell carcinoma syndrome: molecular biology and new hypotheses. Int J Oral Maxillofac Surg 1999 Jun; 28(3): 216-23[Medline]. 7. De Palo G, Veronesi U, Marubini E, et al: Controlled clinical trials with fenretinide in breast cancer, basal cell carcinoma and oral leukoplakia . J Cell Biochem Suppl 1995; 22: 11-7[Medline]. 8. Dzubou LM: Aggressive basal cell carcinoma [letter]. J Am Acad Dermatol 1986 Aug; 15(2 Pt 1): 297-9[Medline]. 9. Etter L, Cook JL: Basal cell carcinoma of the umbilicus: a case report and literature review. Cutis 2003 Feb; 71(2): 123-6[Medline]. 10. Foley P: Clinical efficacy of methyl aminolaevulinate photodynamic therapy in basal cell carcinoma and solar keratosis. Australas J Dermatol 2005 Feb; 45(s2): S8S10[Medline]. 11. Geller AC, Annas GD: Epidemiology of melanoma and nonmelanoma skin cancer . Semin Oncol Nurs 2003; 19(1): 2-11[Medline]. 7 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. Gorlin RJ: Nevoid basal cell carcinoma (Gorlin) syndrome: unanswered issues [editorial; comment]. J Lab Clin Med 1999 Dec; 134(6): 551-2[Medline]. Green CL, Khavari PA: Targets for molecular therapy of skin cancer. Semin Cancer Biol 2004 Feb; 14(1): 63-9[Medline]. Heinritz H, Benzel W, Hoffmann K, et al: Imaging superficial skin tumors of the ENT area. High frequency ultrasound in comparison with computerized tomography and magnetic resonance tomography] . HNO 1995; 43(1): 6-11[Medline]. Horlock N, Grobbelaar AO, Gault DT: Can the carbon dioxide laser completely ablate basal cell carcinomas? A histological study . Br J Plast Surg 2000; 53(4): 28693[Medline]. Humphreys TR, Malhotra R, Scharf MJ, et al: Treatment of superficial basal cell carcinoma and squamous cell carcinoma in situ with a high-energy pulsed carbon dioxide laser . Arch Dermatol 1998; 134(10): 1247-52[Medline]. Kempf RA: Systemic therapy of skin carcinoma. Cancer Treat Res 1995; 78: 13762[Medline]. Lawrence CM: Mohs' micrographic surgery for basal cell carcinoma . Clin Exp Dermatol 1999; 24(2): 130-3[Medline]. Lear JT, Tan BB, Smith AG, et al: Risk factors for basal cell carcinoma in the UK: case-control study in 806 patients . J R Soc Med 1997; 90(7): 371-4[Medline]. Lim JL, Stern RS: High levels of ultraviolet B exposure increase the risk of nonmelanoma skin cancer in psoralen and ultraviolet A-treated patients. J Invest Dermatol 2005 Mar; 124(3): 505-13[Medline]. Ly JQ: Scintigraphic findings in Gorlin's syndrome . Clin Nucl Med 2002; 27(12): 913-4[Medline]. Marks R, Jolley D, Dorevitch AP, Selwood TS: The incidence of non-melanocytic skin cancers in an Australian population: results of a five-year prospective study. Med J Aust 1989 May 1; 150(9): 475-8[Medline]. Mastropasqua MG, Pruneri G, Renne G, et al: Basaloid cell carcinoma of the prostate. Virchows Arch 2003 Dec; 443(6): 787-91[Medline]. Mehta R: Malignant and premalignant skin conditions . Practitioner 2003; 247(1643): 104-7, 109, 112-4[Medline]. Mollenhauer J, Deichmann M, Helmke B, et al: Frequent downregulation of DMBT1 and galectin-3 in epithelial skin cancer . Int J Cancer 2003; 105(2): 149-57[Medline]. Oh CK, Kwon YW, Kim YS, et al: Expression of basic fibroblast growth factor, vascular endothelial growth factor, and thrombospondin-1 related to microvessel density in nonaggressive and aggressive basal cell carcinomas. J Dermatol 2003 Apr; 30(4): 306-13[Medline]. Oster-Schmidt C, Altmeyer P, Stucker M: Successful treatment of basal cell carcinoma on the face with imiquimod 5% cream. Acta Derm Venereol 2002; 82(6): 477[Medline]. Plumb SJ, Argenyi ZB, Stone MS, De Young BR: Cytokeratin 5/6 immunostaining in cutaneous adnexal neoplasms and metastatic adenocarcinoma. Am J Dermatopathol 2004 Dec; 26(6): 447-51[Medline]. Quinn AG, Epstein E: Patched, hedgehog, and skin cancer. Methods Mol Biol 2003; 222: 85-95[Medline]. 8 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. Romao-Correa RF, Maria DA, Soma M, et al: Nucleolar organizer region staining patterns in paraffin-embedded tissue cells from human skin cancers. J Cutan Pathol 2005 May; 32(5): 323-8[Medline]. Saldanha G, Fletcher A, Slater DN: Basal cell carcinoma: a dermatopathological and molecular biological update. Br J Dermatol 2003 Feb; 148(2): 195-202[Medline]. Sharquie KE, Al-Nuaimy AA, Al-Shimary FA: New intralesional therapy for basal cell carcinoma by 2% zinc sulphate solution. Saudi Med J 2005 Feb; 26(2): 35961[Medline]. Smeets N, Neumann M: Mohs' micrographic surgery for basal-cell carcinoma of the face. Lancet 2005; 365(9466): 1227. Smeets NW, Stavast-Kooy AJ, Krekels GA, et al: Adjuvant cytokeratin staining in Mohs micrographic surgery for basal cell carcinoma. Dermatol Surg 2003 Apr; 29(4): 375-7[Medline]. Stockfleth E, Ulrich C, Hauschild A, et al: Successful treatment of basal cell carcinomas in a nevoid basal cell carcinoma syndrome with topical 5% imiquimod. Eur J Dermatol 2002 Nov-Dec; 12(6): 569-72[Medline]. Strauss RM, Edwards S, Stables GI: Pigmented fibroepithelioma of Pinkus. Br J Dermatol 2004 Jun; 150(6): 1208-9[Medline]. Strayer SM, Reynolds PL: Diagnosing skin malignancy: assessment of predictive clinical criteria and risk factors . J Fam Pract 2003; 52(3): 210-8[Medline]. Usatine RP: Recognition for the diagnosis of skin cancer. J Fam Pract 2003 Mar; 52(3): 219-21[Medline]. Wills M: Skin cancer screening. Phys Ther 2002 Dec; 82(12): 1232-7[Medline]. Zimmermann A, Walt H, Haller U, et al: Effects of chlorin-mediated photodynamic therapy combined with fluoropyrimidines in vitro and in a patient. Cancer Chemother Pharmacol 2003 Feb; 51(2): 147-54[Medline]. 9 A basal cell carcinoma, one of the most common types of skin cancer.