Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
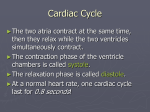
Physio Lab 6: EKG readings by BioPac Today, we will use the school’s laptop computers that have BioPac software installed, and you will see your resting heart rate on an EKG. Then one in your group will go outside and run around for a few minutes and come back to see how that person’s EKG has changed. You will take measurements from the EKG reading to calculate cardiac output. A heart cycle shows up on an EKG as a PQRST segment. P is atrial repolarization Qrs is when the ventricular walls are depolarizing (ventricles are contracting). T is when ventricles are repolarizing (relaxing). Where is atrial repolarization? The electrical activity occurring through ventricle obscures elect activity of atrial repolarization, unless there is a particular abnormal sinus rhythm, then you see it. What is happening after t and before the next p? The heart is completely at rest. If you want water from faucet, turn it on. If you want the water off, turn it off. When the heart contracts, it creates pressure to push blood out. The large elastic arteries expand to allow the large artery to fill up, then the heart rests, but blood continues to flow. Elastic arteries recoil, put pressure on blood, continues to drive blood. On the computer screen, you will see the stroke volume and pulse pressure from your fingertip. You can then calculate the pulse pressure wave velocity. When you are in line at an amusement park and the kids behind you knock you forward, and you bump into the people ahead of you, and they knock the people ahead of them, the line does not speed up; the shock waves just reverberate through the line. Likewise, the blood in elastic arteries bumps the blood ahead of it, and the pulse pressure velocity travels quickly. You will calculate this in lab. Electrical events must precede mechanical events. The instructions below explain the qrs wave; we use the computer to calculate how long the waves take. Delta t means change in time. How long did it take for p wave to occur? You will also need delta t for the segments (flat lines). Intervals include at least one wave. Segments and intervals are measured. When HR increases after exercise, these electrical events shorten a bit, but only so much. The tp part of the cycle should decrease the most. Cardiac output equation: one way to calc is CO= HR x S. V. Skeletal muscles put pressure on veins to bring blood into the heart, and blood must go back out of heart. HR can become so elevated that cardiac output (CO) can decline because the TP segment is short: blood from major veins is returning to heart, bp in atrium is high, the AV valve gets pushed into the ventricle. At rest, 80% of resting is in the atrium. After atria contraction, only 20% more blood is added. If your HR increases too much, you lose your incoming fluid. That means less time for filling, less stroke volume. The heart is filling during resting phase. The heart tissue is getting perfused at the same time. The flaps of the aortic and pulmonary semilunar valves, obstruct the openings of the coronary arteries in the aorta. When the heart relaxes, blood fills the semilunar valves, so it takes time to get blood to the coronary arteries. That increases the risk of heart attack (MI) Do not use USB ports on the side of the computer. There are two on the back; one of those works, not sure which one. If you are plugged into the wrong one in the back, you will not be able to log onto the software and open it up. BioPac: An Introduction To Electrocardiography And Pulse Pressure Waves: Electrical And Mechanical Events Of The Cardiovascular System INTRODUCTION This lab exercise is intended to introduce you to the electrical activity of the heart during the normal cardiac cycle and, by its mechanical contraction (systole), a secondary mechanical event called a pulse pressure wave. You will be generating ECG tracings on a subject within your lab group and making comparisons between various physiological states. The contraction of the heart occurs in order to pump blood out of its ventricles and into the major arteries leading to the lungs and the body. The contraction of the cardiac muscle in both the atria and the ventricles is stimulated to contract by autorhythmic cells that generate the action potential, or depolarization, independent of the nervous system. These “specialized” muscle cells (fibers) are part of the conductive system of the heart, but it is the cells of the sinoatrial (SA) node that are responsible for generating the depolarization wave in a normal heart. This wave of depolarization spreads through the conductive system to the contractile fibers via intercalated discs. The conductive system is a population of specialized fibers that span from the pacemaker cells of the SA node in the right atrium through both atria as bundles, and into the atrioventricular (AV) node in the lower portion of the right atrium. Depolarization along this route causes the contraction of the muscle tissue making up the walls of the atria. The conductive system continues as the bundle of His (AV bundle), fibers leading from the AV node which cross a connective tissue barrier and bring the depolarization to the interventricular septum. It continues into the bundle branches to the apex of the heart and then up the Purkinje fibers. The depolarization wave traveling along this route will depolarize the interventricular septum and the lateral walls of the ventricles. As the depolarization spreads through the ventricle via intercalated disks, it stimulates the contraction of the ventricular muscle tissue. Although the pacemaker cells in the SA node can depolarize on their own, the rate of SA node discharge can be altered by the nervous system. This is accomplished through the autonomic nervous system, originating in the medulla oblongata. Both sympathetic and parasympathetic branches of the ANS tonically discharge, regulating the rate of SA node firing. During a state of arousal or excitement, increased sympathetic nervous system discharge will increase the rate of firing by the SA node and therefore increase the heart rate. At rest, increased parasympathetic nervous system discharge decreases the basal rate of firing by the SA node, subsequently decreasing the heart rate. The electrical activity or depolarization waves through the heart can be recorded using electrodes that cross over the axis of depolarization. By placing a negative electrode on your right wrist and a positive electrode on your left leg, you can measure the current generated on the external surface of the heart as the depolarization moves from the atria to the ventricles. You can also measure the spread of positive charge (or positive current) generated on the surface of the heart during repolarization. The electrical signals can then be used to generate a tracing of the electrical activity of the heart. These tracings are called electrocardiograms, or ECGs (EKGs). The current generated by depolarization of the atria, depolarization of the ventricles and repolarization of the ventricles can all be visualized using these tracings. The standard ECG breaks down into five major waves or peaks: P, Q, R, S, and T. The P wave corresponds to the current created by depolarization of the atria, and is considered the first wave in the cardiac cycle. Q, R, and S are all waves generated by the depolarization of the ventricles, while the T wave generated by the repolarization of the ventricles. The repolarization of the atria is not visible in a normal ECG because the peak is obscured by the simultaneous QRS wave of the ventricle. The amplitude, or height, of each wave is directly proportional to the amount of current occurring during that wave. The duration and amplitude of these waves can be measured clinically to determine whether the heart is acting typically or not. Be aware that these events are electrical in nature and lead to mechanical events that involve muscle contraction. In addition to the typical waves found on an ECG, you can also make various measurements of the time segments between waves. Segments are periods of time between waves while intervals are periods of time including one or more waves. Some of the standard intervals and segments measured include: PR interval: Time between the START of the P wave and the START of the Q wave. Indicates the time it takes for depolarization to reach the ventricles from the SA node and AV delay. PR segment: Time between the END of the P wave and the START of the Q wave. Indicates time through the A V node and this is roughly when the atria would be contracting. ST segment: Time between the END of the S wave and BEGINNING of the T wave. Indicates the time of complete ventricular depolarization and represents when the ventricles would be contracting. QT interval: Time between the START of the Q wave and END of the T wave. Total time of ventricular depolarization and repolarization. TP segment: Time between the end of the T wave and the beginning of the P wave. Indicates the time interval between cardiac cycles. All of these intervals and segments are also used clinically to diagnose changes in the heart activity of a patient. Typical values for the time and amplitude of the waves, segments and intervals are given below, and can be correlated with the speed of the action potential coursing through each region of the heart (GH fig. 10-4 ) Average resting heart rate is approximately 70 beats per minute (bpm.) PHASE P wave PR interval PR segment QRS complex ST segment QT interval T wave DURATION (sec) 0.06-0.11 0.12-0.20 0.08 <0.12 0.12 0.36-0.44 0.16 AMPLITUDE (mV) <0.25 XXXXXXXXXXXXXXX XXXXXXXXXXXXXXX 0.8-1.2 XXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXX <0.5 Now an introduction on the mechanical events that result from the above electrical events: The heart as a pump is designed to generate the force that keeps blood moving through both the systemic and pulmonary circuit. The amount of blood that the heart pumps out of its ventricles per minute is called the cardiac output and is determined by the volume of blood the ventricle (usually the left ventricle) pushes into the large vessels with each contraction, referred to as stroke volume, and the number of times the heart contracts in a minute, the heart rate. Changes in the cardiac output will cause changes in blood pressure and therefore flow rate through the vessels. As blood is pumped into the large arteries of the systemic circuit, the walls of the arteries will stretch and bulge out to accommodate the extra blood. This is due to a large number of elastic fibers found in the walls of the large arteries. As this new volume of blood advances, it will "bump" the neighboring volume of blood farther along in the arterial system, which will then bump another neighboring section farther down and so on. This series of "bumps" is what facilitates blood flow and causes a domino effect of bulging through the arterial system. It is this series of bulging, or the pulse pressure wave, that is felt when a pulse is taken. The velocity of transmission of this wave is about 3 to 5 meters per second along the aorta, and gets progressively faster along smaller arteries. The difference in the velocities is due to the fact that the aorta is more compliant and therefore stretches more while the small arteries are less compliant and transmit the wave much faster. Because of the inertia of the blood, the velocity of the pressure pulse is much greater than the velocity of the actual blood flow. As an example, the pressure pulse velocity is normally about 15 times greater in the aorta than the aortic blood flow. The extent of bulging on the arterial wall, or pulse pressure will change depending on the amount of blood flow to the area. This change may be due to changes in cardiac output as described above, but it may also be due to changes in blood flow to a particular body region. For example, when you are cold, your body will try to keep blood from flowing too close to the surface of the skin to try and prevent heat loss. Because of this, blood flow to your extremities is restricted and the pulse pressure in your fingertips will be low. This will be true regardless of cardiac output. In this exercise, you will be investigating the correlation between the cardiac cycle and the pulse wave generated in your fingertip. Keep in mind as you work that it is the contraction of the left ventricle that initially starts the pulse wave traveling through your systemic circuit and that the pulse wave needs to move from your left ventricle to your fingertip before it can be felt. That means you should expect a time delay between ventricular contraction and pulse pressure in your fingertip. ECG electrodes will be placed on the subject's wrist and ankles, which will then be attached to leads that bring the electrode measurements to the computer. These electrodes will be used to measure depolarizations and repolarizations of the heart. You will also be utilizing plethysmography in order to measure your subject's pulse rate and pulse pressure. This method involves shining a beam of light through the skin of the finger and then measuring the amount of light reflected back. The greater the blood volume (as when blood is being forced into the vessels), the less light is reflected back. These light changes are then converted into an electrical impulse that is sent the computer to generate a graph. The light is generated by an LED and reflected light is measured by a receiver that is attached to your subject's finger. You will also be using the plethysmograph to help measure the velocity (speed) of the pulse pressure wave in your own system. Because we cannot directly determine the exact time when the blood was pushed into the aorta, we will start with the electrical events seen on the EKG. We assume the QRS wave (depolarization of the ventricles) will lead to the mechanical event of the ventricles contracting and, thus, blood ejected into the aorta. The time elapsed from the QRS segment until the NEXT pulse wave reflects the amount of time it required for the pulse pressure wave to reach your finger tip. In order to measure the velocity of this pulse pressure wave, you will have to know the time (in seconds) it takes for the wave to pass from the heart to a particular location on the body (your finger tip). Also, you must determine the distance (in cm) from your heart to that particular body location. The velocity will be calculated by dividing the distance by time to get a velocity in cm/sec. V= D / T EXPERIMENTAL OBJECTIVES 1. To become familiar with the electrocardiograph as a primary tool for evaluating electrical events within the heart. 2. To correlate electrical events as displayed on the ECG with the mechanical events that occur during the cardiac cycle. 3. To observe rate and rhythm in the ECG. NOTE TO STUDENTS: If time runs out, you may download the software from Biopac to analyze your data at home. Simply e-mail your data to your e-mail account and follow these instructions to download the software. See Blackboard/ course documents/ lab units for the actual zip files or use the directions below: Biopac User Software for Data Analysis- Go to http://www.biopac.com/Updates.asp and download the BSL Analysis Only files that correspond to your computer needs. NOTE: if you emailed your data file for analysis to your home computer, the file name may need to be renamed! You'll need to remove the extension before the program will recognize the file. For example, if the file has the extension ".dat" you'll need to remove it, by renaming it. Your file name should read in this form: xxxx-LO7 Windows users. Download the zip folder for the BSL Analysis file to your desktop, extract the files, then click on the .msi file to install software to your computer desktop. MAC Users. This software is for operating systems 10.3 and 10.4. If you have an earlier OS of Mac, you can download the necessary program directly from www.biopac.com/support. You'll need to register for an account (free!) and then download the user software for your computer. Also, you may need the "stuffit Expander" to open the zip file. You can obtain it here: http://www.stuffit.com/mac/expander/download.html For step-by-step directions, this is what a previous student recommends for Mac users: Go to the Biopac website Choose Support - Downloads Choose BSL Analysis Only - 3.7 English - Mac OS You have to register yourself on the Biopac website before it will give you the download link. It then gives you two links, one for the download and another to get Stuffit Expander for free (Mac users only), since you need that program to open the download. When you get directed to the Stuffit Expander site, you have to register with them and they will e-mail you a link to download the program. Once you get the link to the Stuffit download it directs you to the download itself. Choose the trial version at the TOP. There is a much bigger download option at the bottom to get the full version for free, but you have to complete some sort of marketing stipulation. Once you get everything downloaded you should be able to open the e-mailed file from class. You will have to put the file in the Biopac folder first in order to open it though. Now, for the lab PROCEDURE: 1. Have your subject sit on a lab chair or lie down on the lab table. Attach three electrodes to your subject. One on the anterior right wrist and the other two on the medial side of each ankle, just above the medial malleolus. Be sure that the subject does not have socks or shoes that are interfering with the electrodes on the ankles. Also, wrap the pulse transducer around your subject's index finger so that the little box is held tight against the anterior tip of the finger. Make sure it is not so tight that it is restricting blood flow. There is a fine line between tight enough and too tight! Remove any jewelry that may interfere with the recording. 2. Make sure the Biopac unit is turned off and then turn the computer on and log on using login/password. Be mindful of the upper and lower case letters used below for login and password. Computers 1, 3 ,4, 6 and 8: Biology Professor/ Biology Computers 5 and 7: Biology professor/Biology Computer 2: Biology professor/biology Plug the electrode leads into channel 1 on the front of the Biopac unit and the pulse transducer into channel 2 of the unit. Turn the Biopac unit on using the toggle switch on the back of the unit. WAIT for the green busy light to turn off. 3. Attach the white (negative) lead to the wrist electrode on your subject. Attach the black (ground) lead to the right leg electrode and the red (positive) lead to the left leg electrode. Make sure your subject is lying comfortably and quietly, and none of the wires are being pulled. 4. Start the Biopac Lessons program by clicking on the icon found on the desktop. Select lesson "L07-ECG&P-I" from the menu and click OK. You will then be asked to choose a folder for your data. Type your group name and click OK. 5. Calibration-read these instructions FIRST before starting! Make sure the subject's leads are in place and not being pulled on and that the subject is relaxed. It is important whenever you take ECG measurements that your subject does not talk, laugh or move in any way while recording. Click on calibrate and watch the recording while your subject remains relaxed in position. The recording will automatically stop when it reaches the end of the screen. Once finished, check to see that you have both a normal (yet quite reduced) ECG reading and a continuous pulse wave. If not, click on REDO CALIBRATION and try again. You may need to play with the placement and tightness of the pulse transducer, or possibly change fingers, before you get a nice pulse wave. If you are having any problems, ask the instructor. Once your calibration looks good, you may continue on to the next step. 6. Data recording: read first before proceeding! You will be measuring your subject's ECG and pulse under two experimental conditions: Relaxed on the chair or lying on the table and after exercise (note that the Biopac software shows more experimental conditions than what we will do. We will not perform the experiments with hand held over-head nor hand held in ice water—skip these). With your subject resting comfortably, click on RECORD at the top of the data screen and allow the recording to run for 40 seconds (you can follow the seconds on the X-axis of the data screen). Click SUSPEND. If you make a mistake while recording, you may click on REDO and try again. If not, go on to the next step. 7. The computer will automatically place a marker at the top of the data screen every time you click SUSPEND. It appears as a small inverted triangle or a diamond on the upper border of the data screen. Use these markers to decipher between your different experiments. Remember: We will not perform the experiments with hand held over-head nor hand held in ice water—skip these 8. Once you are satisfied with the recording from the resting subject, start the next experiment. In this experiment, you will need to have your subject quickly (!) walk up and down the staircase three times. Keep the electrodes on the subject, but disconnect the wire leads. Immediately after the subject is done, hook them up to the wire leads again and start recording for 40 seconds with the subject sitting or lying comfortably. Expect there to be quite a bit of baseline drift and noise on this one. This is due to the increased respiratory and muscle activity stimulated by the exercise. Click SUSPEND. If you need to repeat the experiment, click REDO. If not, go on to the next step. 9. Click DONE. The screen will ask you what you want to do next. When/ if you are happy with your data, click DONE. If you wish to perform the tests on another subject, select RECORD FROM ANOTHER SUBJECT and pick a second lab partner to gather data from. Repeat all steps for your second subject. You do NOT need to pick a second subject unless you want to analyze more than one person in your group. 10. The screen will again ask you what you want to do next. Select ANALYZE CURRENT DATA from the list and click OK. 11. You may now disconnect your subject from the lead wires, and begin data analysis. Loosely coil the lead wires and replace on table. Do not kink or tangle the wires. DATA ANALYSIS: 1. After you have selected analyze data, the data you recorded will show up in the data screen in a compressed form. The top data window is your ECG data and is denoted as CHI (colored red). The bottom data window is your generated pulse wave and is denoted as CH 40 (colored blue.) Set the channel displays at the top of the screen to read as follows Channel 1 Channel 1 Channel 1 Channel 40 DELTA T-- (displays the time for the selected area) BPM --(calculates heart rate based on one cardiac cycle) p-p (this gives the amplitude of the heart peaks) p-p --(this gives the amplitude of the pulse peaks) 2. In order to analyze your data, you will need to magnify the data. To magnify, click on the magnifying glass in the bottom right hand corner of the data screen. Then, with your mouse, click and drag your mouse from above the upper left of one R wave to below the lower right of another R wave four cardiac cycles down. Before you let go of the mouse button, make sure you have four successive cardiac cycles boxed in. When you release the mouse button, the data screen will be filled with the four cardiac cycles you selected. (Call the instructor over to show you how to do this the first time if you experience any difficulty.) Be sure to take your mouse off of magnifying mode by clicking on the arrow button in the lower right hand side of the data screen. You may still scroll through all of the recordings you did by clicking on the horizontal scroll bar. You may find that you need to have more or less cardiac cycles on the screen in order to reduce background noise and see the waves clearly. 3. At any time during the exercise, if you want to return to seeing all of your waves in a compressed format, click on DISPLAY in the upper toolbar, and click on AUTOSCALE HORIZONTAL in the pull down menu. Also, if your waves are taller than your window height, you can reformat them to fit by clicking on AUTOSCALE WAVEFORMS in the same pull down menu. (The instructor can help you with this if you experience difficulty.) 4. Let’s start with the waves of the ECG and measure their amplitudes and time. The Ch1 p-p measurement box you set up will read amplitude and the DELTA T measurement box will tell you the time. You will now take measurements of the different wave amplitudes and time. Using the I-bar, highlight the region containing the P wave. Be sure you are starting right at the beginning of the P wave and stopping right at the end. Determine the amplitude of the P wave by reading the CH 1p-p box and the time of the P wave by reading the DELTA T box. Record these values in Table 1 on the next page. Repeat this procedure for the QRS complex and the T wave. 5. You now need to take measurements for the time of each of the intervals and segments listed in data table 1 on the following page. Although you only need to take measurements from one cardiac cycle in each experiment, try to choose a cycle that looks pretty average from the beginning of the tracing. Again, to take a reading, highlight the region of the interval or segment you want to measure, making sure to start exactly at the beginning and stop exactly at the end (if you need a review of where these start and stop, see the first two pages of this lab exercise). Read the DELTA T box for the time and amplitudes in Ch1 p-p and record the values in Table 1 provided. 6. Now let’s measure the heart rate, or beats per minute, using your resting data set. Select one cardiac cycle from your data on resting ECG by clicking on the I-bar at the lower right hand side of the data screen. Move your cursor DIRECTLY over the peak of one R wave, click, and drag your mouse to the peak of the adjacent R wave. Be sure you are as exact as possible. The BPM measurement box should now read the calculated beats per minute based on that one cardiac cycle. The delta T should tell you how long that particular cardiac cycle lasted. Write these values in the data chart provided (Table 2). Repeat this process for one more cardiac cycle (R wave-R wave) within the resting data set. Average your two values and write this average in the data chart provided below. 7. Now using the bottom of the screen where the pulse waves are recorded, highlight the area between two successive pulse pressure peaks in your first data set, again being careful about starting and ending the region at the very tip of the peak. Copy the DELTA T and BPM measurements for this selected region (it does not matter that these measurement boxes are set for channel 1). Again, repeat this one more time on different pulse waves and average the data. Record this in table 2. 8. Now determine the amplitude of your QRS waves and pulse waves for your subject while at rest by highlighting one complete QRS wave and copying the CH 1 P-P measurement, then highlighting one complete pulse wave and copying the CH 40 p-p measurement. Again, repeat this one more time and average the data. Record this in table 2. Picking R waves and pulse waves somewhere within the middle of your timed data for a given experiment will give you the best results. 9. Repeat steps 4-8 for the data you collected after exercise. Record all measurements in chart 1 and 2. You can find your exercise data by scrolling through the data on the X-axis of the data screen. 10. Finally, highlight the interval between one R wave and the start of the subsequent pulse wave for each of your data sets. Record the DELTA T in table 3 on the next page. This reflects the time between contraction of the ventricles and the arrival of the pulse pressure wave in your finger. 11. When you are finished, click on File Save As in the tool bar, and save your data in the folder you created at the start of the exercise on the hard drive. This will save your data in your group's file folder. You may always go back to this computer and review your data again by opening the Biopac program, clicking on "review saved data", finding and opening your file in the list, and then clicking on the lab exercise number. Write down the computer’s number here: ________. 12. When done, close the program, turn off the BIOPAC unit using the toggle switch on the back of the unit, then turn off the computer by clicking on the START menu button, and selecting Shutdown. Allow the computer to shut down automatically. Table 1: ECG data Experiment P wave amplitude (mV) P wave time (sec) QRS wave amplitude (mV) QRS wave time (sec) T wave amplitude (mV) T wave time (sec) PR interval (sec) PR segment (sec) ST segment (sec) TP segment (sec) QT interval (sec) Lying down Exercise This one changes the most! TABLE 2: Time Measurements for ECG and pulse waves Condition relaxed After exercise Measurement R-R interval Heart rate Pulse interval Pulse rate Pulse amplitude R-R interval Heart rate Pulse interval Pulse rate Pulse amplitude Channel Delta T BPM Delta T BPM CH 40 P-P Delta T BPM Delta T BPM CH 40 P-P First read Second read Average TABLE 3: Time interval between R wave and pulse wave Condition Delta T person relaxed After exercise QUESTIONS: Use your data and the information given in the introduction to answer the following questions. 1. Is there always a P wave for every QRS complex for your subject? 2. Do the resting (lying down) heart rate and wave durations and amplitudes fall under the normal ranges for your subject? 3. Do the wave amplitudes and durations change very much between lying down and exercise? Would you expect them to? Why or why not? (hint: think sympathetic nervous system). 4. Explain the changes in heart rate between resting and exercising on a molecular level (this is a good time to review the effects of epinephrine on adrenergic receptors of the heart and second messengers). 5. Which of the intervals and/or segments changed the most between resting and exercise? Explain what this tells you about the portion of the cardiac cycle responsible for the increase in heart rate. (Hint: Think about the TP segment and what it represents!) 6. If resting heart rate were compared between two people and one person had an elevated resting heart rate, what could you say about that person’s EDV? SV? And TP segment compared to the person with a lower resting heart rate? 7. What is producing each of the peaks seen in the typical ECG? 8. What mechanical (contractile) event results from each of the peaks seen in the ECG? 9. Using your time data from Table 3, calculate your pulse speed for each of your four conditions: Distance between subject's sternum and shoulder: Distance between subject's shoulder and fingertip : Total distance: cm cm cm Pulse speed = total distance (cm) Time (sec) Pulse speed-arm relaxed Pulse speed-after exercise cm/sec cm/sec 10. Referring to data table 2, how much did the amplitude of the QRS complex change between conditions? What about pulse amplitude? Explain your findings. 11. Which component(s) of the cardiac cycle (atrial systole, atrial diastole, ventricular systole and/or ventricular diastole) is/are directly responsible for the pulse tracing?