Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
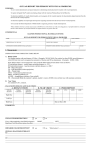
FVE/LMA Report Shell Name: Date of birth: Age: Date(s) of assessment: Evaluator: Title: I. District: Placement/Grade: Date of report: Background Information [Student] is a [age] year old student at [campus] in [district]. [He/she] is currently placed in [placement], and [his/her] primary teacher is [teacher]. This assessment was performed at the request of [requestor] as part of [a three year reevaluation/an initial referral process/other]. II. Eligibility Information Based on the most current report from an eye specialist, and upon the results of this Functional Vision Assessment, [student] [does/does not] qualify as a student with visual impairments under Texas law and current Commissioner’s Rules. III. Medical History A. General Medical records indicate that [student’s] birth history included the following significant components: Significant aspects of [student’s] current medical condition include the following: B. Visual The most current report of an eye exam which is available for [student] is dated [date], and was based on an examination performed by [eye care specialist] of [affiliation or town]. This report indicates that [student’s] visual impairment is due to [diagnosis]. This means that [layman’s definition of diagnosis]. Common educational implications of this condition are: [Student’s] visual acuities using both eyes are listed as: [If no acuities were listed in the report, state the following:] In spite of repeated efforts to obtain visual acuities (or the eye care specialist’s best guess as to visual acuities) for this student, no results in this area were listed on the most current report.] [Student] is currently being [or has previously been] treated for this condition by [treatment –ex. glasses, medications, previous surgeries]. The prognosis for [student’s] condition is that it [prognosis—ex. is stable, is deteriorating, etc.]. C. Other Significant Impairments In addition to [student’s] visual impairment, [he/she] is also impaired in the following ways: These additional impairments tend to affect [student’s] vision in the following ways: [use your resources here, and become an investigator] Developed by Dr. Dixie Mercer – Texas School for the Blind and Visually Impaired – Outreach, 1998. 1 IV. Assessment Environments This Functional Vision Assessment included completing the following steps: 1. a preview observation of the student for [amount of time observed] 2. an analysis of the records in the student’s special education folder 3. three 45 minute observations which took place [list setting for each observation], and 4. a one-on-one testing period which took place in [setting]. Other people present for this assessment included [list others as to their role and function, not their names]. The lighting in the assessment setting was [florescent, incandescent, sunlight, etc.]. [If there were other distractions such as noise, interruptions, etc. note them here.] V. Observation of the Eyes [Student] demonstrated a [positive/negative/very slow] pupillary response to a pen light. This response was [present/not present] in both eyes. [Student] also [demonstrated/did not demonstrate] a blink to threat reflex when an object was unexpectedly moved close to the eyes. The muscle balance of [student’s] eyes was tested by [a confrontation test/coveruncover test] and were found to [list and explain results]. This result indicates that [student] [probably uses/may not use] both of [his/her] eyes together. VI. Visual Acuities A [list type of eye charts] were used to test [student’s] visual acuities at near and distance both with and without glasses. The results of this testing was: [if acuity cannot be measured formally, say so, and delete the chart below, and state something like:] Even though a formal measure of acuity could not be attained, [student] demonstrated that [he/she] did have some vision. VII. Visual Fields Visual field testing was done with [student] by [list method]. The results of this testing indicated that [student] [probably does not/may] have a significant field limitation. [Use if appropriate] This field limitation appears to be [describe location]. [Student’s] most effective visual field appears to be [describe location]. VIII. Ocular Motility Several activities were performed in order to assess the efficiency with which [student] could move [his/her] eyes. These include: [list activities]. Specifically, an effort was made to assess the effectiveness of [student’s] ability to: Visually fixate – look at an object and keep [her/his] eyes locked on the target, Track – use [his/her] eyes to follow a moving target without moving the head, Scan – sweep [her/his] eyes across the environment to locate a visual target, and Focal shift – rapidly and efficiently move [his/her] eyes from one visual target to another. Results from the tests listed above indicated that [student] has the following ocular motility capabilities. Developed by Dr. Dixie Mercer – Texas School for the Blind and Visually Impaired – Outreach, 1998. 2 Visually fixate – [Student] [is/is not] able to maintain [his/her] eyes on a specific visual target. Track -- [Student] [is/is not] able to smoothly move [his/her] eyes in order to follow a specific visual target through space. [Explain any tracking deviations noticed.] Scan -- [Student] [is/is not] able to sweep [his/her] eyes across the environment in order to locate a specific visual target. [Explain any scanning deviations noticed.] Focal shift -- [Student] [is/is not] able to move [his/her] eyes from one visual target to another. IX. Color Perception In order to assess [student’s] color perception, [he/she] was asked to perform several tasks. These included: [list tasks]. [Student’s] performance on these tasks indicated that [he/she] [does/does not] likely have trouble distinguishing colors. [Explain any problems noticed.] [If no testing of Color Perception was done, say so and why.] X. Visual Abilities In order to get a better idea of the functional implications of [student’s] visual impairment, [he/she] was asked to locate a number of small objects at various points in space. These tasks can be categorized as near, intermediate, and distance vision abilities. Results were: Near – [list the smallest object that the student could see and give the distance at which it was seen. Ex. “Matt was able to see a cake decorating bead at two inches when presented on a contrasting background.”] Intermediate – [see above] Distance – [see above] XI. Visual Motor The ability to coordinate visual input with movement is critical for many tasks students are asked to perform in school. Therefore, [student] was asked to do several visual motor activities. These included [list activities]. At the fine motor level, [student] was able to [summarize performance on fine motor tasks]. On gross motor tasks, [student] was able to [summarize performance on gross motor tasks]. In general, [no/a good deal] of [over/under reaching] was observed. This indicates that [student] [is/is not] always sure of the location of visual targets in space and [may/probably does not] have significant problems with depth perception. XII. Learning Media Assessment A. Sensory Modalities Observation during the course of this Functional Vision Assessment indicates that the sensory modality which [Student] seems to use most efficiently is [his/her] [visual, tactual, or auditory] system. The secondary sensory modality seems to be [vision, tactual, or auditory]. B. Reading [Student] currently uses primarily [braille/large print/regular print] as [his/her] primary literacy medium. [She/he] is currently reading on the [grade] level at a rate of [number] words per minute. A list of low vision devices used includes: [list devices]. Using these devices [student] is able to read: [device] – [number] words per minute Developed by Dr. Dixie Mercer – Texas School for the Blind and Visually Impaired – Outreach, 1998. 3 [device] – [number] words per minute [device] – [number] words per minute During this assessment, [student] was able to read [number] point print. [He/she] was also able to read [list all that apply with distance --telephone book print/ newspaper print/regular print/large print/etc.] at a distance of [number] inches. [Provide any other relevant information on reading.] C. Writing Currently, [manuscript/cursive/braille writer/keyboarding] is [student’s] primary writing medium. [He/she] is able to write approximately [number] words per minute when [explain testing method]. [Student] uses the following adaptive materials for writing: [list – including dark lined paper, dark pens, etc.]. [She/he] [is/is not] able to keyboard at this time. D. Audio Visual [Student] reports having difficulty with the following audio visual equipment when it is used in the classroom: [list – VCR, overhead, films, television, blackboard, etc.) XIII. Conclusion/Educational Implications In summary, the following are the educational implications which are likely to result from [student’s] visual impairment: [list] [list] XIV. Recommendations Based on an analysis of the records available, interviews with [student’s] parents and teachers, and the assessment reported here, the following recommendations are made: 1. [Student] [should/should not] receive an Orientation and Mobility evaluation. [state why] 2. [He/she] [should/should not] receive a Low Vision assessment from a low vision specialist. [state why] 3. Further testing of [student’s] functional vision capabilities [should/should not] be undertaken at this time. [State why, for example: the information gained was sufficient at this time - or – not sufficient, and more testing is needed. If more assessment is needed, when should it be done? Who should do it? What areas should be explored?] 4. [List recommendations of TVI services – Consult or Direct, how many minutes per week or month, or however your particular district wishes them written.] 5. [List recommendations in the compensatory areas: daily living skills, social skills, career and vocational, technology, etc. Should more assessment be done in these areas?] 6. [List recommendations regarding the Full Individual Evaluation. What tests should be used? What techniques are appropriate? What adaptations should be made?] 7. [List recommendations for adaptations of disaster drills.] 8. [List Modifications that need to be made based on the information in this report. It has truly been a pleasure to assess [student], [Write a couple of sentences about what you like best about this student. Emphasize his or her strengths.] Developed by Dr. Dixie Mercer – Texas School for the Blind and Visually Impaired – Outreach, 1998. 4 ____________________________________________ Name of evaluator Title District Phone number Developed by Dr. Dixie Mercer – Texas School for the Blind and Visually Impaired – Outreach, 1998. 5