Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Auditory processing disorder wikipedia , lookup
Hearing loss wikipedia , lookup
Sound localization wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
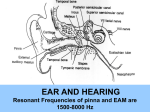
Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 1 of 23 INNER EAR PHYSIOLOGY AND PATHOLOGY Resources Nolte The Human Brain: An introduction to its functional anatomy Chapter 14 Hearing and Balance: The eighth cranial nerve Auditory transduction animation (LRC) Inner ear case Differential diagnosis and treatment of hearing loss Issacson and Vora paper CRITICAL FACTS (if med school is a Minnesota forest with millions of trees, these are the red pines). 1. Inner ear receptors are divided into two types; both types convert mechanical energy into receptor potentials. TYPE I (INNER HAIR CELLS) are the true sensory receptors that convey information to the brainstem. TYPE II (OUTER HAIR CELLS) function as biological amplifiers, essentially acting as motor units. 2. Inner ear transduction is DIRECTIONAL: displacement toward the tallest stereocilia (positive deflection) results in DEPOLARIZATION. In the cochlea, this occurs when the basilar membrane moves toward scala vestibuli. Negative deflection (toward scala tympani) results in HYPERPOLARIZATION. 3. The SEMICIRCULAR CANALS detect head rotation (angular acceleration). The OTOLITH ORGANS (UTRICLE and SACCULE) detect gravity (linear acceleration). The vestibular system is involved in balance and posture, co-ordination of head and body movements and in fixating the visual image on the fovea. 4. SEMICIRCULAR CANALS WORK IN PAIRS. HORIZONTAL CANALS: depolarization occurs in the SAME direction as the head rotation. A/P CANALS: depolarization occurs in the OPPOSITE direction as the head tilt. The natural pairing is of LEFT ANTERIOR with RIGHT POSTERIOR CANAL (and vice versa). Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 2 of 23 5. The VESTIBULO-OCULAR REFLEX is a 3 neuron arc (hair cell/vestibular nerve, vestibular nuclei, cranial nerve motor nuclei) that is used to adjust eye position to compensate for changes in head position (i.e., it keeps the visual image centred on the fovea). Remembering the pairings listed in fact #4, there is depolarization / excitation / contraction in one of the pathways of the pair, and hyperpolarization / inhibition / relaxation in the other. Rotation of the head in one direction results in rotation of the eyes in the opposite direction. 6. There are two systems responsible for vestibulospinal reflexes. The LATERAL VESTIBULOSPINAL SYSTEM is responsible for postural changes to compensate for tilts and movements of the body. The MEDIAL VESTIBULOSPINAL SYSTEM stabilizes head position during walking. The two systems differ with respect to their afferent source, vestibular nucleus connections, efferent projections, how they produce their effect on neck and trunk muscles and their control mechanisms. 7. The middle ear transfer function determines the absolute threshold of hearing at each frequency in normal individuals – the cochlea is so sensitive, it can transduce any signal that reaches it. This implies that anything that alters middle ear function (like an infection) will significantly impact hearing thresholds. 8. Sound waves pass through the cochlea INSTANTANEOUSLY. The traveling wave pattern on the basilar membrane is established more gradually and is INDEPENDENT of how the motion is initiated i.e., don't need to deliver sound via the oval window --- can use bone! The traveling wave establishes a frequency vs. place relationship along the length of the cochlea, with high frequencies being transduced in the base, and low frequencies in the apex. 9. Outer hair cells use their receptor potential to exert force on the basilar membrane ---thereby generating a POSITIVE FEEDBACK MECHANISM which amplifies the vibration of the membrane in a nonlinear, highly frequency specific manner. This force produces its own fluid wave, which is conducted back through the perilymph, vibrating the middle ear apparatus and generating sounds that are emitted from the ear (OTOACOUSTIC EMISSIONS). 10. The STRIA VASCULARIS produces the endolymph (high K+) and the endocochlear potential (+80 mV). Many of the ion transporters of the Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 3 of 23 stria are the same as those in the kidney, so drugs that affect renal function are often ototoxic – esp. loop diuretics (which affect the Na+/K+/2Cl- transporter). 11. Sounds are localized by the differences in timing and intensity between the two ears. Lateral superior olive (LSO) neurons localize high frequency stimuli by comparing interaural intensity differences (IIDs); medial superior olive (MSO) neurons use interaural timing differences (ITDs) to localize low frequency stimuli. 12. NYSTAGMUS consists of a slow drift of the eyes in one direction (PURSUIT) followed by a rapid recovery movement in the opposite direction (SACCADE). The direction is named for the fast component i.e., a RIGHTWARD NYSTAGMUS consists of slow movement of eyes to the left, followed by fast recovery to the right. The PURSUIT is controlled by vestibulo-ocular reflex; the SACCADE by higher centers (e.g., cortex). 13. The caloric test can be used to assess brain function. In a person with a normally functioning cortex, injection of cool water into the right ear, will produce a LEFTWARD NYSTAGMUS (COLD=OPPOSITE COWS). If the patient is COMATOSE, the SACCADE WILL BE ABSENT (the VOR, which operates in the brainstem is still functional and the pursuit will be intact). If the patient is BRAIN DEAD, both the PURSUIT and SACCADE WILL BE ABSENT. 14. There are three types of hearing loss: CONDUCTIVE: external or middle ear SENSORINEURAL: inner ear, auditory nerve or cochlear nucleus MIXED: conductive and sensorineural 60% of sensorineural hearing losses (the most severe type) are due to genetic factors, and 40% to environmental factors. As the U.S. population ages, this distribution will change. 15. Because of the extensive bilateral connections of the auditory system, the only way to have an ipsilateral hearing loss from a single lesion is to have a peripheral defect i.e., at the cochlea, auditory nerve or cochlear nucleus Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 4 of 23 bilateral hearing loss from a single lesion is invariably due to a lesion located centrally N.B. Noise exposure, ototoxic drugs and congenital malformations can cause simultaneous damage bilaterally but these are considered to be multiple lesions. 16. Ménière’s disease is characterized by intermittent spells of severe vertigo and nystagmus, fluctuating hearing loss and tinnitus. This disease has an unknown etiology, and there is no universally successful treatment. ESSENTIAL MATERIAL FROM OTHER LECTURES (i.e., things you should know before you get to this lecture) 1. Anatomy of the external and middle ears: pinna, tympanic membrane, middle ear ossicles (malleus, incus, stapes), middle ear muscles (tensor tympani, stapedius), round and oval windows 2. Histology of the cochlea: inner and outer hair cells, stereocilia, basilar membrane; scalae vestibule, tympani and media; tectorial membrane, stria vascularis 3. Histology of the vestibular labyrinth: type I and type II hair cells, utricle, saccule, semicircular canals, cupula, ampulla, cristae, striola, otoliths 4. Hair cell ultrastructure: subcellular cisternae 5. Auditory pathways: auditory nerve, cochlear nucleus, superior olivary complex, inferior colliculus 6. Vestibular pathways: vestibular nerve, lateral, medial and superior vestibular nuclei, III and VI cranial nerve nuclei 7. Descending control of spinal reflexes (Dr. Stauffer) 8. Neurological exam: Rinne and Weber tests stereocilia, kinocilium, cuticular plate, reticular lamina, LEARNING OBJECTIVES (i.e., the things that I will be testing you on!) 1. Describe the structural features of hair cells that are critical to their function. Identify key similarities and differences between type I and type II hair cells. 2. Explain the tip link model of transduction. In particular, be able to describe the generation of a biphasic receptor potential and adaptation. 3. Contrast the semicircular canals and otolith organs with respect to: a) the mechanism of stereocilia displacement, b) directionality and c) the type of effective stimulus. Describe the natural pairing of semicircular canals, and be able to indicate which canals are depolarized/hyperpolarized by specific head movements. Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 5 of 23 4. List the steps in the vestibulo-ocular reflex and describe the changes in firing patterns in each nucleus during head rotation. Identify the function of the VOR. 5. Compare and contrast the anatomical and physiological aspects of the medial and lateral vestibulospinal systems with respect to: overall function, afferent source, vestibular nucleus, efferent projections and effect and control mechanism. 6. Describe how the mass and stiffness characteristics of the middle ear affect sound transmission. List the mechanisms used by the middle ear to minimize the impedance mismatch between air and the cochlear fluids. Graph and be able to interpret the audiograms generated in patients with normal hearing, a conductive hearing loss and sensorineural hearing loss. 7. Outline how a traveling wave is established on the basilar membrane in response to an acoustic stimulus. Define the cochlear place code and describe how it is established via the passive properties of the basilar membrane and organ of Corti. 8. Diagram the active feedback mechanism invoked by contraction of the outer hair cells. Identify the difference between otoacoustic emissions and tinnitus. Identify the source of OAE, and describe how they can be used to derive an audiogram (e.g., during newborn hearing screenings). 9. Describe the generation of the endocochlear potential (EP) and its function. Understand the impact on hearing of interfering with the EP (e.g., with loop diuretics). 10. Compare the pathways and mechanism for localizing low and high frequency stimuli. Be able to describe the physiology underlying the Rinne and Weber tests. 11. Define nystagmus, and understand its origins (i.e., which part is due to VOR, and which to higher centers). Describe the differences in caloric nystagmus among a normal individual, a comatose patient and in a person who is brain dead. 12. Be able to define the terms: prelingual and lingual deafness, conductive and sensorineural hearing loss, central auditory processing disorder, presbycusis and tinnitus. 13. Compare and contrast the symptoms and treatment of acoustic neuromas and Ménière’s disease. Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 6 of 23 HAIR CELL TRANSDUCTION There are two types of inner ear receptors; both types convert mechanical energy into receptor potentials. TYPE I (INNER HAIR CELLS) are the true sensory receptors that convey information to the brainstem. TYPE II (OUTER HAIR CELLS) function as biological amplifiers, essentially acting as motor units. Structure/Function Relationships TYPE I TYPE II Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 7 of 23 Transduction Mechanism Inner ear transduction is DIRECTIONAL: displacement toward the tallest stereocilia (positive deflection) results in DEPOLARIZATION. In the cochlea, this occurs when the basilar membrane moves toward scala vestibuli. Negative deflection (toward scala tympani) results in HYPERPOLARIZATION. Tip Links & Transduction Channels Adaptation Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 8 of 23 BALANCE Components The SEMICIRCULAR CANALS detect head rotation (angular acceleration). The OTOLITH ORGANS (UTRICLE and SACCULE) detect gravity (linear acceleration). The vestibular system is involved in balance and posture, co-ordination of head and body movements and in fixating the visual image on the fovea. Semicircular Canals Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 9 of 23 SEMICIRCULAR CANALS WORK IN PAIRS. HORIZONTAL CANALS: depolarization occurs in the SAME direction as the head rotation. A/P CANALS: depolarization occurs in the OPPOSITE direction as the head tilt. The natural pairing is of LEFT ANTERIOR with RIGHT POSTERIOR CANAL (and vice versa). Otolith Organs Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Vestibular Reflexes Vestibulo-Ocular Reflex Winter 2009 Inner Ear Physiology and Pathology Page 10 of 23 Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 11 of 23 Vestibulospinal Reflexes There are two systems responsible for vestibulospinal reflexes. The LATERAL VESTIBULOSPINAL SYSTEM is responsible for postural changes to compensate for tilts and movements of the body. The MEDIAL VESTIBULOSPINAL SYSTEM stabilizes head position during walking. The two systems differ with respect to their afferent source, vestibular nucleus connections, efferent projections, how they produce their effect on neck and trunk muscles and their control mechanisms. LATERAL VESTIBULOSPINAL TRACT (LVST) AFFERENT SOURCE VESTIBULAR NUCLEUS entire labyrinth (motion and gravity) semicircular canals (motion) lateral vestibular (Dieter's nucleus) to medial aspects of laminae VII and VIII medial and descending vestibular nuclei to MLF ipsilateral bilateral excitatory excitatory and inhibitory see Dr. Forbes lectures EFFERENT CONNECTIONS EFFERENT EFFECT CONTROL MECHANISM see Dr. Stauffer's lecture on Descending control or this review of spinal reflexes MEDIAL VESTIBULOSPINAL TRACT (MVST) adjustment of proximal limb and trunk musculature by: 1. contraction of extensor muscles via direct excitation of alpha and gamma motor neurons (mechanisms 1 and 4) 2. indirect relaxation of flexor muscles via excitation of inhibitory interneurons (mechanism 2) relaxation of muscles of upper back and neck 1. direct inhibition of alpha motor neurons (mechanism 1) IT IS UNDOUBTEDLY MUCH MORE COMPLICATED THAN THIS!!! Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html HEARING Acoustics Middle Ear Function Winter 2009 Inner Ear Physiology and Pathology Page 12 of 23 Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 13 of 23 Impedance matching Acoustic impedance The middle ear transfer function determines the absolute threshold of hearing at each frequency in normal individuals – the cochlea is so sensitive, it can transduce any signal reaches it. This implies that anything that alters middle ear function (like an infection) will significantly impact hearing thresholds. Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 14 of 23 Audiograms Basilar Membrane Deflection Sound waves pass through the cochlea INSTANTANEOUSLY. Traveling Wave & Place Principle The traveling wave pattern on the basilar membrane is established more gradually and is INDEPENDENT of how the motion is initiated i.e., don't need to deliver sound via the oval window --- can use bone! The traveling wave establishes a frequency vs. place relationship along the length of the cochlea, with high frequencies being transduced in the base, and low frequencies in the apex. Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 15 of 23 Passive Properties Active process Outer hair cells use their receptor potential to exert force on the basilar membrane ---thereby generating a POSITIVE FEEDBACK MECHANISM which amplifies the vibration of the membrane in a nonlinear, highly frequency specific manner. This force produces its own fluid wave, which is conducted back through the perilymph, vibrating the middle ear apparatus and generating sounds that are emitted from the ear (OTOACOUSTIC EMISSIONS). Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 16 of 23 Otoacoustic emissions Endocochlear Potential & Stria Vascularis The STRIA VASCULARIS produces the endolymph (high K+) and the endocochlear potential (+80 mV). Many of the ion transporters of the stria are the same as those in the kidney, so drugs that affect renal function are often ototoxic – esp. loop diuretics (which affect the Na+/K+/2Cl- transporter). Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Central Processing Pathways Auditory Brainstem Responses Winter 2009 Inner Ear Physiology and Pathology Page 17 of 23 Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 18 of 23 Sound localization Sounds are localized by the differences in timing and intensity between the two ears. Lateral superior olive (LSO) neurons localize high frequency stimuli by comparing interaural intensity differences (IIDs); medial superior olive (MSO) neurons use interaural timing differences (ITDs) to localize low frequency stimuli. Hearing Tests for details on tympanometry, Rinne/Weber and audiograms (behavioural, ABRs, OAEs), please look at my Website Audiograms Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 19 of 23 INNER EAR PATHOLOGY Vestibular only Nystagmus NYSTAGMUS consists of a slow drift of the eyes in one direction (PURSUIT) followed by a rapid recovery movement in the opposite direction (SACCADE). The direction is named for the fast component i.e., a RIGHTWARD NYSTAGMUS consists of slow movement of eyes to the left, followed by fast recovery to the right. The PURSUIT is controlled by vestibulo-ocular reflex; the SACCADE by higher centers (e.g., cortex). The caloric test can be used to assess brain function. In a person with a normally functioning cortex, injection of cool water into the right ear, will produce a LEFTWARD NYSTAGMUS (COLD=OPPOSITE COWS). If the patient is COMATOSE, the SACCADE WILL BE ABSENT (the VOR, which operates in the brainstem is still functional and the pursuit will be intact). If the patient is BRAIN DEAD, both the PURSUIT and SACCADE WILL BE ABSENT. Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 20 of 23 Benign positional vertigo Labyrinthitis (A&V?) Auditory only Hearing Loss There are three types of hearing loss: CONDUCTIVE: external or middle ear SENSORINEURAL: inner ear, auditory nerve or cochlear nucleus MIXED: both 60% of sensorineural hearing losses (the most severe type) are due to genetic factors, and 40% to environmental factors. As the U.S. population ages, this distribution will change. Genetics Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Conductive Hearing Loss Sensorineural Hearing Loss Cochlear Implant Winter 2009 Inner Ear Physiology and Pathology Page 21 of 23 Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 22 of 23 Because of the extensive bilateral connections of the auditory system, the only way to have an ipsilateral hearing loss from a single lesion is to have a peripheral defect i.e., at the cochlea, auditory nerve or cochlear nucleus bilateral hearing loss from a single lesion is invariably due to a lesion located centrally N.B. Noise exposure, ototoxic drugs and congenital malformations can cause simultaneous damage bilaterally but these are considered to be multiple lesions. Central Processing Disorders (CAPD) Tinnitus Presbycusis Med 6573 Nervous System Dr. Janet Fitzakerley [email protected] http://www.d.umn.edu/~jfitzake/Lectures/Teaching.html Winter 2009 Inner Ear Physiology and Pathology Page 23 of 23 Vestibular and Auditory Acoustic Neuroma Ménière’s Disease Ménière’s disease is characterized by intermittent spells of severe vertigo and nystagmus, fluctuating hearing loss and tinnitus. This disease has an unknown etiology, and there is no universally successful treatment.