Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Dentistry throughout the world wikipedia , lookup
Dental hygienist wikipedia , lookup
Dental degree wikipedia , lookup
Dental implant wikipedia , lookup
Special needs dentistry wikipedia , lookup
Impacted wisdom teeth wikipedia , lookup
Scaling and root planing wikipedia , lookup
Periodontal disease wikipedia , lookup
Focal infection theory wikipedia , lookup
Tooth whitening wikipedia , lookup
Remineralisation of teeth wikipedia , lookup
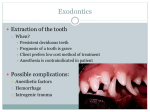
Endodontic therapy wikipedia , lookup
Crown (dentistry) wikipedia , lookup
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA BANGALORE PROFORMA FOR REGISTRATION OF SUBJECTS FOR DISSERTATION 1. NAME OF THE Dr. ANUBHAV AGARWAL CANDIDATE AND POST GRADUATE STUDENT ADDRESS DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY, COLLEGE OF DENTAL SCIENCES , DAVANGERE – 577 004, KARNATAKA. 2. NAME OF THE COLLEGE OF DENTAL SCIENCES INSTITUTION DAVANGERE – 577 004 KARNATAKA 3. 4. COURSE OF STUDY MASTER OF DENTAL SURGERY (M.D.S), AND SUBJECT ORAL & MAXILLOFACIAL SURGERY DATE OF ADMISSION 31th MAY 2012 TO COURSE 5. TITLE OF THE TOPIC “ PHYSICS FORCEPS VERSUS CONVENTIONAL FORCEPS FOR TOOTH EXTRACTION: A COMPARATIVE STUDY ” 6. BRIEF RESUME OF THE INTENDED WORK: 6.1 Need for the Study: Tooth extraction is a traumatic procedure often resulting in immediate destruction and loss of alveolar bone and surrounding soft tissues which leads to complex cascade of biochemical and histological events then ensues during the wound healing process which further leads to physiologic alterations to alveolar bone and soft tissue architecture. One such atraumatic extraction technique using the ‘PHYSICS FORCEPS’ can reduce the degree of damage and extent of resorption that physiologically occurs following tooth extraction. Extraction socket with an undamaged alveolus and well preserved soft tissues can be successfully treated with post extraction procedures like immediate implant placement or fixed partial denture. 6.2 REVIEW OF LITERATURE: This article reviews and highlights exodontia tips as well as new techniques to make simple and complex exodontia more predictable and with improved patient outcomes. This article have a brief discussion on physics forceps, a new type of exodontia forceps, which uses class 1 lever mechanics to extract teeth without having to use excessive force or squeezing motion, on basic and complex exodontia.1 This article deals with technological advances in extraction techniques. The physics forceps used first-class lever mechanics to atraumatically extract a tooth from its socket. One handle of the devices is connected to a bumper, which act as fulcrum during the extraction. This bumper is usually placed on the facial aspect of the dental alveolus, typically at mucogingival junction. The beak of the extractor is positioned most often on the lingual or palatal root of the tooth and into the gingival sulcus. Unlike conventional forceps, only one point of contact is made on the tooth being extracted. A squeezing motion should not be used with these forceps. By contrast, the handles are actually rotated as one unit using a steady yet gentle rotational force with wrist movement only. Once a tooth is loosened, it may be removed with traditional instruments such as conventional forceps or rongeur.2 In this article the author has evaluated a new extraction method for intentional replantation. Many authors emphasize that safe extraction without crown or root fracture is the primary prerequisite for successful intentional replantation. However many teeth indicated for intentional replantation are weakened by repetitive root canal treatments and root canal post. Moreover, molar tooth require a significant amount of load during extraction due to broad root surface, curved and divergent roots also make fracture-free safe extraction difficult. Nonetheless, little is known about the practical extraction method for intentional replantation, except that an elevator should not be used and the beak of the conventional forceps should be placed on the crown above cemento-enamel junction. Atraumatic safe extraction using newly developed physics forceps along with preoperative orthodontic treatment has been introduced recently. The aim of their study was to evaluate the reliability of atraumatic safe extraction for intentional replantation.3 This article deals with assessment and classification of extraction defects. Tooth extraction is a traumatic procedure resulting in immediate destruction and loss of alveolar bone and surrounding soft tissue. The clinical presentation of alveolar defects seen immediately following tooth removal varies from simple to complex. This evaluation can only be accurately made immediately following extraction, since damage often occurs during the process of tooth removal. A classification of extraction the extraction defect, as it presents immediately following tooth removal associated with dental implant treatment recommendations would be beneficial for the clinician in establishing the most appropriate plan for treatment. This paper presents a novel extraction –defect classification system which categorizes extraction defects and provide guidelines for dental implant treatment.4 This article states about biomechanical rational for atraumatic tooth extraction. Biomechanical aspects of force have been applied to tooth extraction for centuries. However, the mechanical advantages available to extract the tooth were primarily applied to hold the crown of the tooth, rather than extract it. An extraction device physics forceps has been developed to apply a biomechanical rational to the extraction process of a tooth using a class 1 lever, creep and shear component of force. The physics forceps is really a dental extractor than a forceps and uses first-class lever mechanics. Creep is a phenomenon whereby a material continues to change shape over time under a constant load. In tooth extraction, creep may occur in bone and periodontal ligament. Under a constant load of 60 Mega pascals, the bone over time changes shape in three different stages. This action contributes to the creep rupture of the ligament and usually elevates the tooth few millimeters from socket. At this point the tooth is loose and ready to be removed from the socket using conventional extraction forceps. When a rotating force is applied to the physics forceps on the tooth, the stress to the tooth and periodontal complex is a shear component of force. The force applied to the gum and bone by the bumper is over a greater surface area and is a compressive force, thus bracing the buccal bone. This permits the lingual plate to expand more and protects the facial plate from fracture.5 6.3 AIMS & OBJECTIVES OF THE STUDY: •The purpose of this study is to evaluate the effectiveness of physics forceps over conventional forceps in atraumatic dental extraction. •The purpose of this study is to compare the advantages and disadvantages of physics forceps over conventional forceps. The ‘PHYSICS FORCEPS’ are an innovative design that provides the simple mechanical advantage by employing first class lever mechanics . 7. MATERIAL AND METHODS: 7.1 SOURCE OF DATA: 200 patients referred for extraction reporting to department of Oral and Maxillofacial Surgery, college of dental sciences, davangere will be selected for the study with their informed consent. 7.2 METHODOLOGY: i. Two hundred patients will be categorised in two groups : GROUP I: extraction in 100 patients using the conventional extraction technique will be considered as control group for the study. GROUP II: extraction in 100 patients using the PHYSICS FORCEPS. ii. In group 1 patients, extraction will be done using the conventional extraction technique. In group II patients, extraction will be done using the new extraction technique, the physics forceps. iii. Both the extraction defects in these groups will be assessed with the use of an extraction defect sounding classification system. The extraction defect sounding classification system describes the condition of the hard as well as soft tissues immediately following tooth removal, prior to healing and remodeling of the extraction socket. This classification only applies after the treatment decision has been made to remove a tooth and an objective evaluation of the extraction defect is made. The time required during extraction of tooth with physics forceps and conventional extraction technique will also be compared. 7.3 CRITERIA FOR THE SELECTION : INCLUSION CRITERIA Firm tooth which are indicated for extraction. Patients who requires immediate implant placement. Grossly decayed tooth. Tooth that requires intentional replantation. Tooth that are indicated for open extraction. EXCLUSION CRITERIA Patients having systemic illness. Patients who have periodontally compromised tooth. 7.4 METHOD OF STATISTICAL ANALYSIS: The data will be collected and statistically analyzed. 7.5 DOES THE STUDY REQUIRE ANY INVESTIGATIONS OR INTERVENTIONS TO BE CONDUCTED ON PATIENTS OR OTHER HUMANS OR ANIMALS? IF SO PLEASE DESCIBE BRIEFLY. Yes, Intra oral periapical radiograph of concerned tooth need to be taken. 7.6 HAS ETHICAL INSTITUTION : Yes CLEARANCE BEEN OBTAINED FROM YOUR 8. LIST OF REFERENCES: 1) Harry Dym, Adam Weiss. Exodontia: Tips and techniques for better outcomes. Dental Clinics of North America. 2012; 56:245-266. 2) Adam Weiss, Avishai Stern. Technological Advances in Extraction Techniques and Outpatient Oral Surgery. Dental Clinics of North America. 2011; 55:501-513. 3) Choi YH, Bae JH. Clinical evaluation of a new extraction method for intentional replantation. Journal of Korean Academy of Conservative Dentistry. 2011; 36(3):211217. 4) Nicholas Caplanis, Jaime L Lozada, Joseph YK Kan. Extraction Defect: Assessment, Classification and Management. International Journal of Clinical Implant Dentistry, 2009; 1(1):1-11. 5) Carl E Misch, Helena M Perez. Atraumatic extractions: A Biomechanical Rationale. Dentistry today, 2008; 27(8):100-1. 9. SIGNATURE OF THE CANDIDATE 10. REMARKS OF THE GUIDE 11. NAME AND DESIGNATION OF 11.1 GUIDE DR. MANJUNATH S. M.D.S. PROFESSOR , DEPARTMENT OF ORAL ANDMAXILLOFACIAL SURGERY, COLLEGE OF DENTAL SCIENCES, DAVANGERE-577004 11.2 SIGNATURE 11.3 CO-GUIDE ( IF ANY) 11.4 SIGNATURE 11.5 HEAD OF THE DEPARTMENT 11.6 SIGNATURE 12. 12.1 REMARKS OF THE CHAIRMAN AND PRINCIPAL 12.2 SIGNATURE DR. K.S.N. SIVA BHARANI M.D.S. PROFESSOR AND HOD, DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY, COLLEGE OF DENTAL SCIENCES, DAVANGERE-577004