Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
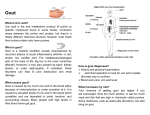
GOUT Presented by Group 4 Stephanie Choi Carlos Garcia Manolito Gulla Stacy Hirabayashi Maria James-Howell Joseph Oni Carol Quintyne Lorna Smith Domingo Templonuevo GOUT I. Introduction As student nurses and future primary caregivers, we all should be properly educated to be able to bring optimum care to our clients, and gout, which has an increasing trend of occurrence in both men and women, should not be looked over. Gout which also known as metabolic arthritis is a disease due to an inborn uric acid metabolism. In this condition sodium urate crystals are deposited on the articular cartilage of the joints and in the particular tissue like tendons. A primary risk factor for gout is hyperuricemia – high levels of uric acid in the blood. People who have this are at risk of having an attack of gout. But the condition usually develops because the kidneys cannot eliminate enough uric acid from the blood. This provokes an inflammatory reaction of these tissues; these deposits often increase in size and burst through the skin to form sinuses discharging a chalky white material. A gout “flare” (attack) usually strikes suddenly at night, in one location (usually the large joint in the big toe). During the attack the area becomes hot, red, swollen, and extremely tender. A fever may also be present. The pain, can be excruciating, usually peaks within 24 hours. No one can predict when an attack might occur for someone with hyperuricemia. It may be triggered by alcohol, certain medicines, the presence of another illness (diabetes), stressful events or some other factors. With or without treatment, the symptoms usually go away within 3 to 10 days, and the next attack may not occur for months or even years, if at all. However, over time attacks can become more severe, last longer, and occur more often. There may be a genetic link: many people with the condition have a family history of gout. Adult men, particularly those between the ages of 40 and 50 are more likely to develop gout than women. Most women experience gout after menopause and have other medical conditions, such as high blood pressure causing kidney problems, and are taking medication that affects their body’s ability to keep uric acid levels low. II. Dietary Treatments and Rationale In people who have Gout, uric acid production in the body is increased while elimination is reduced. Uric acid is a substance that result from the breakdown of purines, which are found in all human tissues and in many of the foods we eat. This causes pain and swelling in the affected joints. Consequently, one way of treating Gout is through dietary alteration. The American Medical Association recommends a diet that is : 1. High in complex carbohydrates. That is, fiber-rich whole grains, fruits and vegetables. Rationale: Fiber assists with elimination and weight control. 2. Low in protein. That is, only 15% of calories should come from protein. Sources should be soy, lean meats or poultry. Rationale: to reduce purine intake 3. No more than 30% of calories in fat, with only 10% being from animal fat. Rationale: to promote weight loss and reduce purine intake. 4. Also recommended is a higher than normal intake of fluid, such as unsweetened fruit juice, unsweetened diluting drinks, full/semi skimmed milk, tea and coffee. Rationale: May assist with excretion of uric acid through renal tubes Recommended foods are: - Fresh cherries, strawberries, and other red-blue berries - bananas - celery - tomatoes - vegetables including kale, cabbage, parsley, green-leafy vegetable - foods high in bromelain ,such as, pineapple - foods high in vitamin C, such as, red cabbage, red bell peppers, tangerines , mandarins, oranges, potatoes - low fat diary products - complex carbohydrates, such as, bread cereals pasta, rice , vegetables and fruits - chocolate , cocoa - coffee , tea - carbonated beverages - essential fatty- acids such as tuna, salmon, flaxseed, nuts, seeds - Tofu may be a good replacement for meat, but legumes and things made from soybeans are also good choices. Although, purine is found in all protein foods it is not recommended that all purine sources be eliminated from the diet. III. Socioeconomic and Cultural Factors of the Diet Gout has been recognized since antiquity, and according to some researchers, “Gout is sometimes referred to as the ‘disease of kings’ due to its high occurrence in royal families, and their high consumption in rich foods and overindulgence in wine. However, the general consensus among modern researchers is that gout appears to be more prevalent in countries that have a high standard of living, and since obesity is one of the contributing factors of the disease, it is safe to say that Western countries are affected more than others. In addition, it appears that the cultural factors of the diet compounded by genetic factors are equally or more compelling than the socioeconomic factors in predisposing one to the disease. According to the National Institutes of Health “gout affects approximately 2.1 million people in the United States, and is predominantly a disease of adult men over age 40.” Moreover, that same report made strong assertions that African American men are more at risk for gout than their Caucasian counterparts. However, in an article entitled Worldwide Prevalence and Observations, it was brought out that Black Africans, Japanese, and Native Americans have significantly lower levels of gout than the Caucasian population, and that same article says “Multiple studies over the past 40 years have provided data consistent with a considerable increase in prevalence and annual incidence in Westernized industrialized countries.” In a similar vein, studies show that “A family history of gout is common for those who develop the disease, and this may be a result of genetic predisposition or environmental factors. Patterns of gout within families ranging from 11-80% have been reported, and two large series found that 40% of gout patients had a family history of gout.” If these reports are all conclusive, that does not bode well for African Americans. It is reported that heavy consumption of alcohol, obesity, hypertension, hyperlipidemia, diabetes, and sickle cell anemia are all contributing factors of gout, and sad to relate the African American population has a high incidence of these diseases. Moreover, a diet high in fat and cholesterol and rich in purines and organ meats are also a part of the African American diet (something that text books have deliberately excluded). Therefore, it is logical to conclude that African Americans would be at a high risk for gout. However, if environmental factors are also culprits in this disease anyone could be susceptible. Gout has been rare in countries such China, Polynesia, and the Philippines. But studies show that when people born in these countries move to areas with a higher standard of living, their incidence of gout has also tended to increase. This strongly suggests that environmental factors may play a role (perhaps a minor role) in gout. Of course, more studies have to be done on this, but all of the evidence points to the fact that industrialized countries have a high incidence of gout. They also suggest that the socioeconomic and cultural factors of the diet make African Americans vulnerable to the disease. IV. Patient Teaching and Rational for Dietary Concerns Teaching the client about gout is a form of nursing intervention which is a part of the nursing process. Consequently, the first step in the nursing process is assessment wherein, in this case we need to critically examine each piece of information related to gout such as lifestyle, diet, alcohol consumption, weight, and other risk factors associated with uric acid build-up that triggers gout attack. We may also look for the medical history, blood tests results, and vital signs that may suggest other conditions related to this disease. We need a good critical thinking skills and a systematic method of assessment to correctly pinpoint the actual and potential problem and to be able formulate an effective plan of managing these problems through patient teaching. The main goal of patient teaching is to successfully educate the client to be able to understand the risk factors, the cause and effect of the disease, and to convince the client to change and accomplish certain objectives going towards wellness. “Gout is believe to be an inherited metabolic disorder and there is no known cure, however through healthy lifestyle, proper diet and right medication, symptoms maybe relieved and painful episodes could be eliminated” (www.gout.com, Friendlyfoods p. 1) If the gout episode is triggered by high level of purines in the diet, the client has to learn to identify those foods to be avoided and the right ones to be consumed. We may also look into the client’s alcohol consumption that could likewise trigger an episode, and the client should be advised to avoid alcoholic beverages if necessary. One common concern regarding dietary intervention is that the patient is forced to eat foods that are not part of his usual diet. For example, the patient feels that he is being given “American” food. Therefore, nurses and dietitians should take into account cultural aspects of the diet. The menu should take the patients usual food preferences then adding and subtracting elements in order to reduce the amount of its purine content. The following is the Mount Sinai Hospital Modified Gout diet (Low-Sodium} which can be used as a model in teaching the client the proper diet: Include in Each Day’s Diet Milk Meat Cheese Egg Bread Cereal Potato or substitute Vegetables Fruit or fruit juices Jam or sugar Butter Coffee or tea Chicken Roast beef Roast veal Roast lamb Chops: Lamb Veal Veal cutlet 1 pint or less 4 ounces 1 ounce of salt free pot cheese only 1 only 6 slices or less of salt free or matzoh only ½ cup or less 1 portion 3 portions as desired 4 teaspoon or less 2 teaspoons or less of sweet butter only as desired. Meat Portion (4 ounces) Selected from the Following: 1 medium breast or leg 1 medium slice 1 medium slice 1 medium slice 2 medium rib or 1 shoulder 1 loin (1/2” thick} 1 piece 5” x 2 ½ x 1/2 Other “risk factors for gout associated conditions include obesity, high blood sugar, hypertension, elevated cholesterol level” (Meg Sibal, M. D.), and should be assessed and evaluated properly, and if necessary educate the client about weight management through proper exercise and healthy lifestyle. In addition, alternative ways to manage this painful gout disease must also be taught to the client to provide him/her an option such as “prevention of gout attacks with the use of drugs, allopurinol designed to normalize uric acid levels by slowing down the rate of uric acid production, administration of colchicin and/or the non-steroidal anti inflammatory drug (NSAID) which can alleviate the acute pain and inflammation” (M. Sibal}. After teaching the client about gout, the next step in the process is to document what was done and evaluate, and measure the effectiveness of the teaching process. If for some reason, the patient teaching did not work effectively, we have to modify the plan. D. Medication Classifications and Two Prototype Drugs Colchicine are tablets that are used to prevent or treat the attacks of gout. Colchicine is therapeutic and it is an antigout agent. This drug can be taken in two different dosages: the larger dose is used for acute attacks of gouty arthritis and a smaller dosage is used in the prevention or the recurrence of gout. It is believed that the pain involves colchicines major pharmacological action: binding to tubulin dimers. Tubulin is a protein consisting of two forms, alpha and beta. Alpha and beta tubulin form dimers, and these dimers polymerize to form long filaments of microtubules. When colchine binds to the tubulin dimers, the dimers are unable to form microtubules. The microtubules are vital for formation of spindle fibers during mitosis and meiosis, intracellular transport of vesicles and proteins, flagella reassemble, amoeboid motility and other processes. Inhibition of amoeboid motility prevents macrophage and leukocyte migration and phagocytes, thereby presumably preventing the inflammation and pain of gout. What this actually sums up to mean is that the medication colchicines disrupts mitosis, thereby halting the process of metaphase, which is involved in the process of gout formation. Anti-inflammatory drugs such as Colchinine are used to treat gout. They are effective in alleviating the acute symptoms of gout. However, they do not stop uric acid synthesis nor promote uric acid excretion. Therefore the cause of gout is still there. In 1963, a new drug for treatment of gout was marketed. Allopurinol (Zyloprim) is a uric acid inhibitor. It inhibits the formation of uric acid and therefore lowers uric acid levels in the blood. The formation of uric acid is inhibited because the drug inhibits the enzyme xanthine oxidase which is needed in the synthesis of uric acid. Allopurinol goes right down into the very cause of the disease and therefore is effective in treating chronic gout. It comes under the Medical Classification of Anti-Gout: uric acid inhibitor drug. Contraindications: it should not be given to patients with severe renal disease. When taking this drug, increased fluid intake is recommended to promote urination. Dosage: for adults PO initially 100 mg/day, may increase to 200-300 mg/day for mild gout and 400600 mg/day for severe gout. Maximum is 800mg/day. Side effects include anorexia, nausea, vomiting, diarrhea, dizziness, headache, rash, itching, depression, and metallic taste. Bibliography Kee, Joyce LeFever, and Evelyn Hayes. Pharmacology:A Nursing Process Approach. New York: W. B. Saunders Company, 2002. Mount Sinai Hospital Modified Gout Diet (Low-Sodium, 2005) Sibal, M. “M.D. 2006”. The Filipino Reporter (New York). 10-19 October 2006: 49-50 www.gout.com-Friendly foods (2005) www.healthnotes.com www.healthcastle.com www.podiatrychannel.com/gout/index.shtml