Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
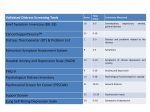
Cancer Center Administrators Forum March 31, 2015 Jeanine Stiles Chief Administrative Officer Associate Director for Administration ONE HEALTH, ONE VISION Lost in Transition After Cancer “The medical system that saved my life wasn’t able to help me not want to take my life… I have developed a deep love and reverence for the oncologists and nurses, and I believe that these people really do understand that, in some ways, it never ends for us. But I also believe that collectively the system of care failed to prepare me for the mental health crisis that I would experience.” “There’s no excuse for that.” “While an increasing number of cancer treatment centers have begun offering post-treatment care plans and support groups to help patients navigate these challenges, many patients continue to fall through the cracks. “Sometimes we do a good job of preparing people for this, but often we don’t,” Dr. Oeffinger said. “We need to do a better job.” ONE HEALTH, ONE VISION Building Supportive Oncology/Psycho-Oncology Programs “We like to think of the end of cancer treatment as the closing of a chapter, but what most people don’t realize is that the emotional struggle continues long after,” Dr. Kevin C. Oeffinger, a primary care physician and director of Memorial Sloan Kettering Cancer Center’s adult long-term follow-up program, told me recently over the phone. “Feelings of post-treatment depression and anxiety are amazingly normal. I would go so far as to say that if you don’t have them it’s a surprise.” Suleika Jaouad Cancer Survivor Full story New York Times: Lost in Transition After Cancer: http://mobile.nytimes.com/blogs/well/2015/03/16/lost-in-transition-after-cancer ONE HEALTH, ONE VISION It’s the Right Thing to do for Patient Centered Care Commission on Cancer New Standards for ACoS Accreditation • Patient Navigation Process - 3.1 • Distress Screening - 3.2 • Survivorship Care Plan - 3.3 The importance of identifying and addressing supportive care needs of cancer patients is widely recognized as a core component of high-quality cancer care. The IOM asserts that “...health care systems that are involved in cancer care should explicitly incorporate attention to psychosocial needs into their policies, practices and standards (Adler).” Despite this, supportive care needs of cancer patients too often go undetected and untreated. The IOM concludes that cancer care delivery systems in the US are in crisis. ONE HEALTH, ONE VISION UCDCCC – Other NCI Designated Cancer Centers ONE HEALTH, ONE VISION UCDCCC Staff Satisfaction % of Staff Satisfied or Very Satisfied Staff Satisfaction Survey Overall GOAL Staff Support Meeting needs Access to care 0% 20% 40% 60% 80% 100% • Overall staff satisfaction rate was 29% • Staff satisfaction rate goal is 90% • Dissatisfaction was highest around issues of patient access to supportive care. ONE HEALTH, ONE VISION It takes a Team Angie Usher, LCSW Jena Cooreman, LCSW Jeanine Stiles, CAO Julie Giannini, RN Nathan Fairman, MD ONE HEALTH, ONE VISION The Journey City Of Hope Training 3 day workshop Matthew J. Loscalzo, L.C.S.W. Executive Director, Supportive Care Medicine Administrative Director, Sheri & Les Biller Patient and Family Resource Center Liliane Elkins Professor in Supportive Care Programs, Endowed Professor Professor, Population Sciences Lots of Homework to do….. ONE HEALTH, ONE VISION Internal Partnerships Department of Psychiatry/Hematology-Oncology/ Primary Care/Public Health Sciences – Support of a Psychiatric Clinic within the Cancer Center – Joint recruitment of Psycho/Oncologist – current recruitment – Buy in from Medical Oncologist – Partnerships with primary care MD’s for Survivors Clinic – Education vehicle for primary care MD’s – Outcomes Research in concert with Public Health Sciences ONE HEALTH, ONE VISION Making the Case Distress Screening Pilot • A 6-month, IRB approved, distress screening pilot study of 358 Cancer Center patients was completed in February 2014. • Screening Tool: National Comprehensive Cancer Network Distress Thermometer and adapted problem checklist • Process: – Patients rate their current level of distress on a scale from 0 to 10 – Causes of distress assessed using 39-item problem checklist – Patients scoring 5 or above referred to social services for assessment ONE HEALTH, ONE VISION Results of Screening Pilot 38% 40% 0-2 minimal distress 3-4 moderate distress 5-10 high to severe distress % reporting a problem Reported Distress Levels n=358 Frequency of Reported Problems for patients with high to severe distress n = 136 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 82% 82% Emotional Problems Physical Problems 60% 35% Practical Problems Family Problems Problem Area 22% 38% of patients reported high to severe levels of distress 30% were referred to social services 38% of patients reported high to severe levels of distress 30% were referred to social services Current staffing (1.75 FTE) meets approximately 10.5% of the need for psychosocial services among highly distressed new patients. ONE HEALTH, ONE VISION Focus Groups Cancer Survivors’ Focus Group • April 2014 - focus group of cancer survivors was conducted with the following goals: – Identify common areas of concern among cancer survivors – Use information to guide development of survivorship care • Most prevalent emergent themes included concerns about: – – – – access to supportive care services, care coordination between different services provision of emotional support Supportive care services felt to be of high quality but insufficient to meet patient need ONE HEALTH, ONE VISION Why Invest – Benefits to Patient • Reduced emotional distress and improved quality of life (Faller et. al., 2013) • Improved patient and family communication and coping skills (Graves, 2003) • Reduced barriers to patient care • Improved patient investment in and acceptance of diagnosis, treatment goals and prognosis • Increased access to community supportive resources ONE HEALTH, ONE VISION Why Invest – Benefits to Providers • Addressing the psychosocial needs of distressed clinic patients in real time allows physician to maintain clinic schedule with minimal disruption • Assistance in communicating information to patients and families • Filters distractions from disease-specific care • Easily accessible, dependable compassionate experts who help patients and support doctors • Address complex psychosocial problems for which doctors do not have time or training ONE HEALTH, ONE VISION Why Invest – Benefits to Health System • Brings UCDHS into alignment with national standards / guidelines for quality cancer care • Models several goals of the UCDHS Strategic Plan • Reduces healthcare costs and increases revenues – Psychotherapeutic interventions correlated to subsequent reduction in health care use. Reductions are more prominent for high utilizers (Lane; Sobel; Crane, et al) – Cancer patients with mild to significant mood disturbance have increased utilization rates of hospital care and can raise medical costs up to 250% (Carlson & Bultz) – A meta-analytic review of the impact of psychological interventions on health care utilization, found an average 20% savings resulting from psychological interventions (Chiles, et al) – Cost of providing therapeutic interventions has been shown to be offset by medical cost savings over time (Lechnyr; Guthrie, et al) ONE HEALTH, ONE VISION FTE Requested Proposal Submitted to Health System Leadership December 2014 Supportive Oncology Services: Requested Additional Staffing Staff 2014 FTE current staff 2015 FTE request Psychiatrist 0.2 0.4* Adult LCSW 1.75 3.0 Nurse Practitioner 2016 FTE request Total FTE request 2.0 5.0 1.0 Adult RD 0.6 1.4 Pediatric LCSW 0.5 0.5 1.0 2.0 3.4 0.5 Pediatric RD 0.4 0.6 1.0 Child Life Specialist 1.0 1.0 Practical Assistance Coordinator 1.0 1.0 Total of 13 FTE’s requested ONE HEALTH, ONE VISION Survivorship A report last year by the American Cancer Society, in collaboration with the National Cancer Institute, estimates there are almost 14.5 million cancer survivors alive in the United States today, and that number will grow to almost 19 million by 2024. Although more and more Americans are surviving cancer thanks to early detection programs, new treatment regimens and awareness campaigns, much remains to be learned about the short- and long-term issues faced by survivors. With long-term survival comes a new challenge: how to keep cancer survivors healthy and emotionally stable after treatment ends. ONE HEALTH, ONE VISION Establishing A Survivors Clinic • Provide patients the environment to address and deal with latent side affect, emotional support, Not lost in Transition • Develop survivorship care plans – EMR tool. • Allow oncologist to see newly diagnosed • MD champion in survivor issues and side affects • Ability to develop a robust program for outcomes research • External advisor for survivor issues • External advisor for Health Services Research • Hiring of a dedicated QA RN ONE HEALTH, ONE VISION Implementation Plan YEAR 1: • Design and develop a module in EMR for data capture of distress and nutrition screening • Design and implement supportive oncology plan of care • Communicate importance of supportive oncology services to patients and family • Create a survivorship clinic to address end-of-treatment needs and assist in transition to primary care • Develop practical assistance services to quickly and efficiently address concrete patient needs • Identify psychosocial needs of new patients through distress screening • Identify nutritional needs of new patients through routine screening • Create clear clinical pathways to supportive care services • Provide supportive oncology education to providers and staff • Identify opportunities for community partnerships to improve access to services and resources ONE HEALTH, ONE VISION Implementation Plan YEAR 2: • • • • • • Conduct follow-up, reevaluation and adjustment of supportive oncology plan of care Expand distress screening to include follow-up screening at pivotal points of treatment Expand nutritional screening to include follow-up patients Continue to increase access to services through internal development and community partnerships Introduce psychotherapy services for patients utilizing LCSW staff in lieu of licensed psychologists Quality oversight ONE HEALTH, ONE VISION How We Will Measure Our Impact • A Project to Assure Quality Cancer Care (APAQCC) • UCDCCC has been accepted as a participant to this research project being conducted by the Association of Oncology Social Work • The purpose of this project is to: – Improve the psychosocial care received by cancer patients and their families – Provide social workers with tools and skills to implement and monitor psychosocial care, particularly distress screening, and adhere to standards of care (American College of Surgeons, QOPI) – Inform Social Work practice and provide data to advocate for resources (e.g., programmatic support, staffing) • Participants in APAQCC will: – Assess their institution’s capacity for providing psychosocial support services and compare it to other similar institutions – Use data for quality improvement and enhancement of support service delivery ONE HEALTH, ONE VISION Drinks with Shrinks ONE HEALTH, ONE VISION Kentucky Has Nothing Over California ONE HEALTH, ONE VISION